

Probing SARS-CoV-2-positive plasma to identify potential factors correlating with mild COVID-19 in Ghana, West Africa
- PMID: 36184636
- PMCID: PMC9527094
- DOI: 10.1186/s12916-022-02571-2
Probing SARS-CoV-2-positive plasma to identify potential factors correlating with mild COVID-19 in Ghana, West Africa
Abstract
Background: West Africa has recorded a relatively higher proportion of asymptomatic coronavirus disease 2019 (COVID-19) cases than the rest of the world, and West Africa-specific host factors could play a role in this discrepancy. Here, we assessed the association between COVID-19 severity among Ghanaians with their immune profiles and ABO blood groups.
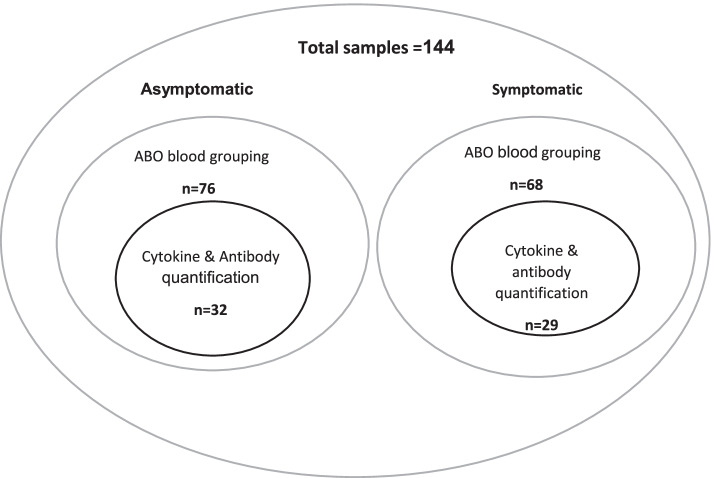
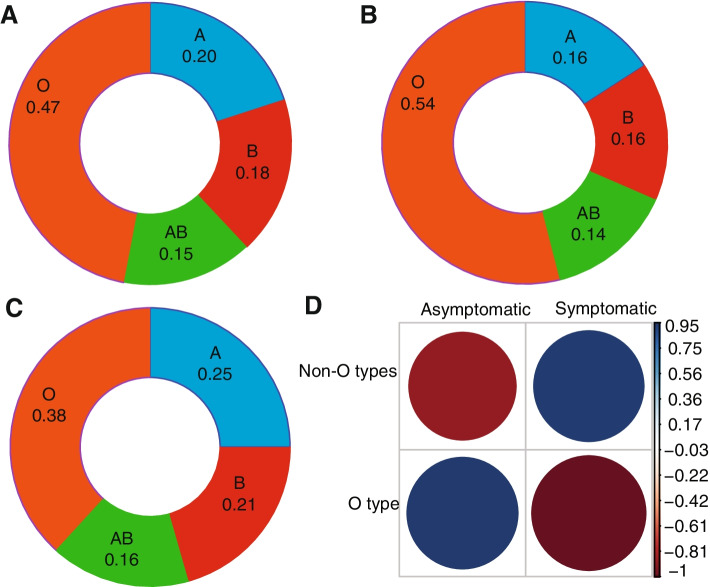
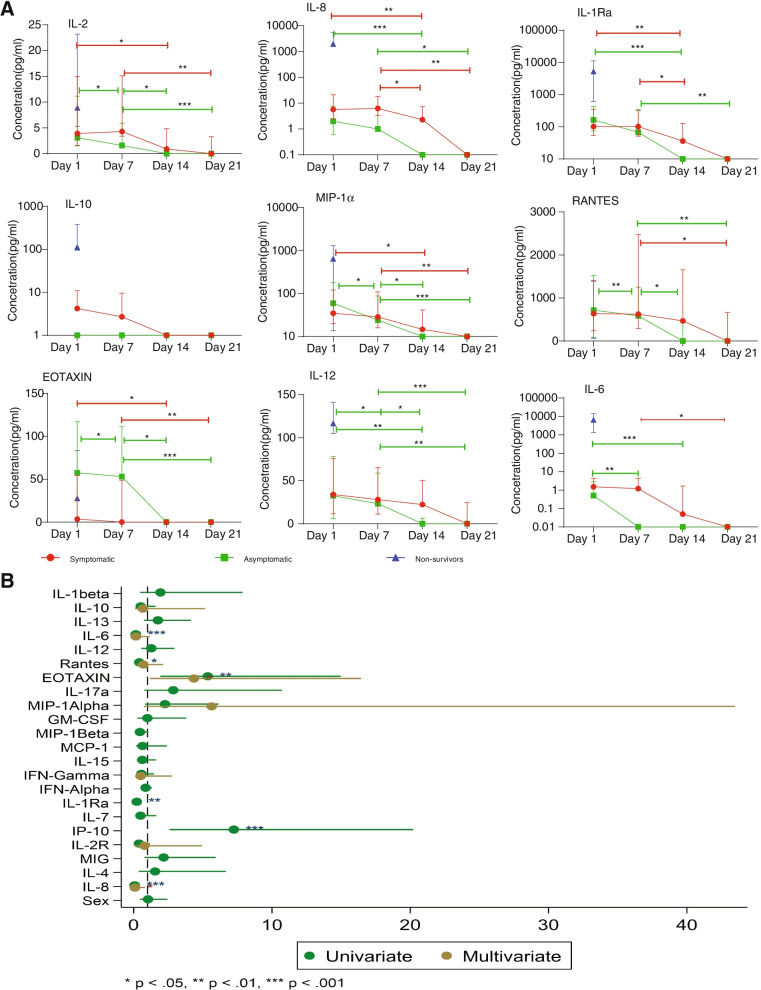
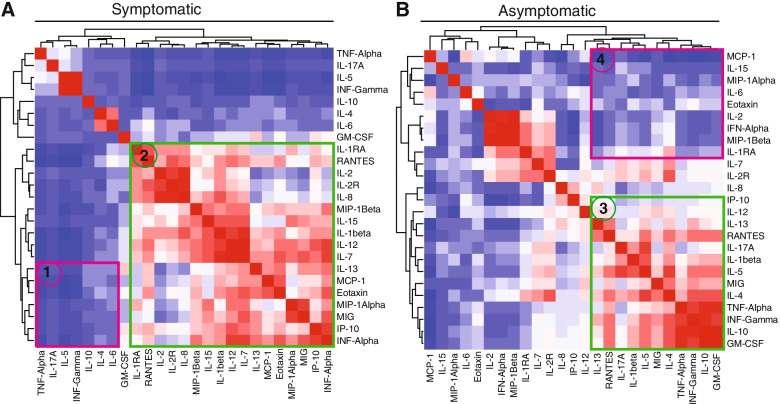
Methods: Plasma samples were obtained from Ghanaians PCR-confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-positive individuals. The participants were categorized into symptomatic and asymptomatic cases. Cytokine profiling and antibody quantification were performed using Luminex™ multiplex assay whereas antigen-driven agglutination assay was used to assess the ABO blood groups. Immune profile levels between symptomatic and asymptomatic groups were compared using the two-tailed Mann-Whitney U test. Multiple comparisons of cytokine levels among and between days were tested using Kruskal-Wallis with Dunn's post hoc test. Correlations within ABO blood grouping (O's and non-O's) and between cytokines were determined using Spearman correlations. Logistic regression analysis was performed to assess the association of various cytokines with asymptomatic phenotype.
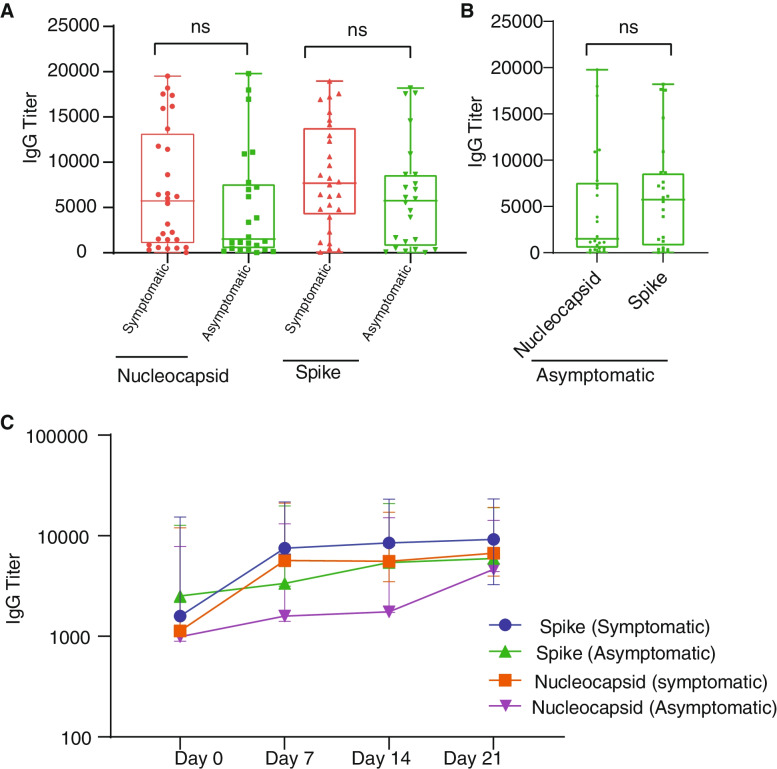
Results: There was a trend linking blood group O to reduced disease severity, but this association was not statistically significant. Generally, symptomatic patients displayed significantly (p < 0.05) higher cytokine levels compared to asymptomatic cases with exception of Eotaxin, which was positively associated with asymptomatic cases. There were also significant (p < 0.05) associations between other immune markers (IL-6, IL-8 and IL-1Ra) and disease severity. Cytokines' clustering patterns differ between symptomatic and asymptomatic cases. We observed a steady decrease in the concentration of most cytokines over time, while anti-SARS-CoV-2 antibody levels were stable for at least a month, regardless of the COVID-19 status.
Conclusions: The findings suggest that genetic background and pre-existing immune response patterns may in part shape the nature of the symptomatic response against COVID-19 in a West African population. This study offers clear directions to be explored further in larger studies.
Keywords: ABO blood groups; Antibodies; Asymptomatic; COVID-19; Eotaxin; West Africa.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- WHO . WHO coronavirus (COVID-19) dashboard. 2021. pp. 1–6.
-
- Worldometers . Coronavirus cases. Worldometers.info; 2022. pp. 109–112.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
