

doi: 10.1016/j.eats.2022.05.002.
eCollection 2022 Sep.
Patellar Tendon Imbrication for the Treatment of Patella Alta in Skeletally Immature Patients
Affiliations
- PMID: 36185114
- PMCID: PMC9519932
- DOI: 10.1016/j.eats.2022.05.002
Item in Clipboard
Patellar Tendon Imbrication for the Treatment of Patella Alta in Skeletally Immature Patients
Arthrosc Tech.
.
Abstract
Patella alta is a major contributor to recurrent patellar instability, which is commonly seen in young athletes. Distalizing tibial tubercle osteotomy has been used for the correction of patella alta and patellar instability, but this procedure is contraindicated in the skeletally immature patient population, as it could lead to growth arrest of the proximal tibial physes. We propose a patellar tendon imbrication technique as a soft-tissue alternative to tibial tubercle osteotomy. When used with concomitant medial patellofemoral ligament reconstruction, we suggest this procedure may prove beneficial for the treatment of patellar instability in skeletally immature patients.
© 2022 The Authors.
Figures
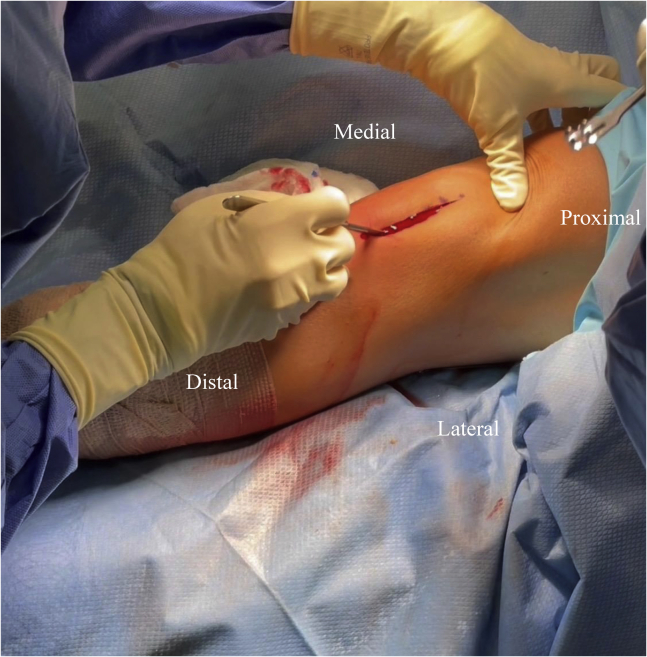
This image shows the patient placed in the supine position. On the left knee, an anterolateral parapatellar incision is made and the iliotibial band is released from the capsule. This will allow for suspensory fixation of the medial patellofemoral ligament, access to the patellar tendon, and access to the medial aspect of the patella by retracting the patella laterally.
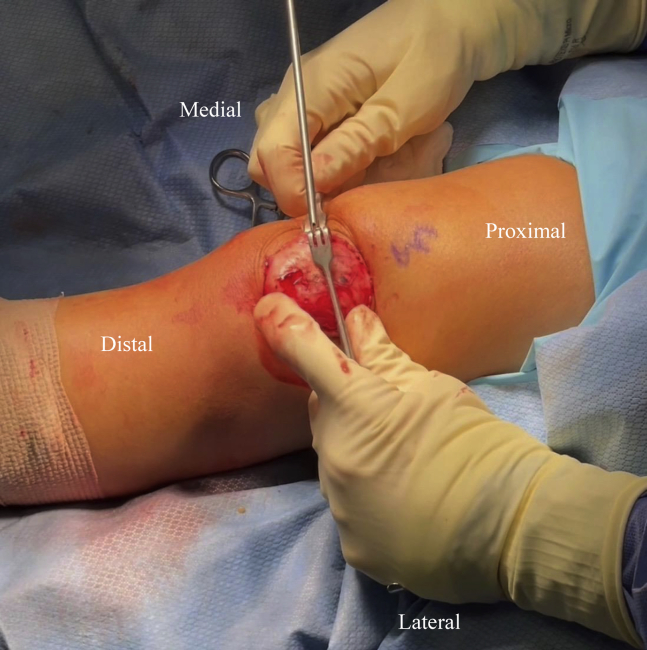
This image shows the patient placed in the supine position. On the left knee, the patella is retracted laterally to allow for placement of the suture anchors. Two 1.8-mm Q-FIX anchors (Smith & Nephew) are placed along the medial aspect of the patella. The first anchor is placed approximately at the midpoint of the patella and another is placed 5 mm proximally.
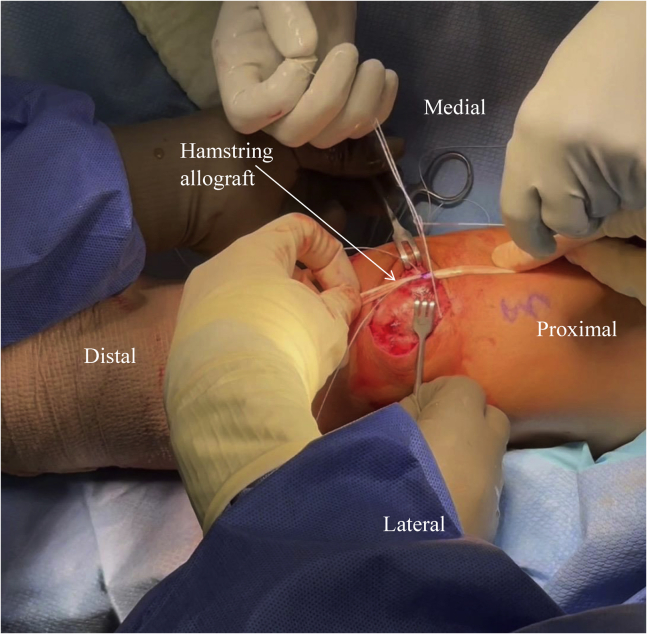
This image shows the patient placed in the supine position. On the left knee, a hamstring allograft is marked at the midpoint and tied down using the sutures from the 2 anchors along the medial aspect of the patella.
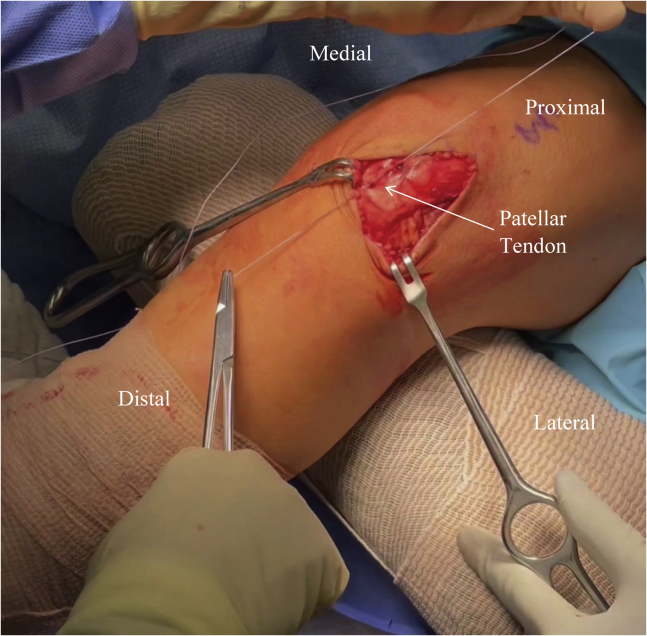
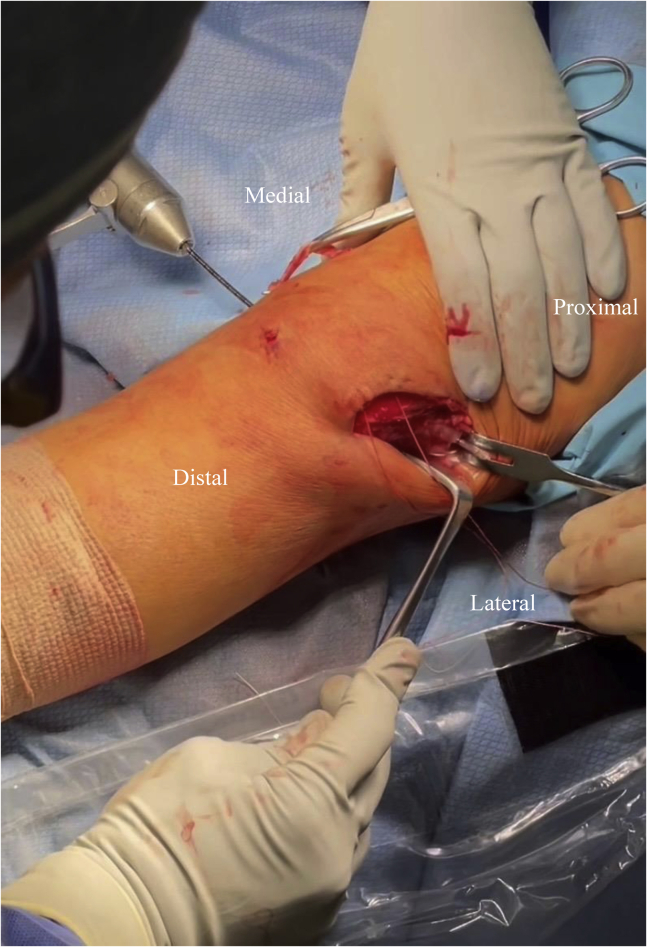
This image shows the patient placed in the supine position with their left knee positioned on a padded bump with about 30° of flexion. Two retractors are used to hold open a lateral parapatellar incision to allow sufficient access for the patellar tendon imbrication. The completion of the first figure-of-eight suture is shown along the medial patellar tendon. Upon completion of the 7 figure-of-eight sutures, the patellar tendon is shortened by 1 cm.
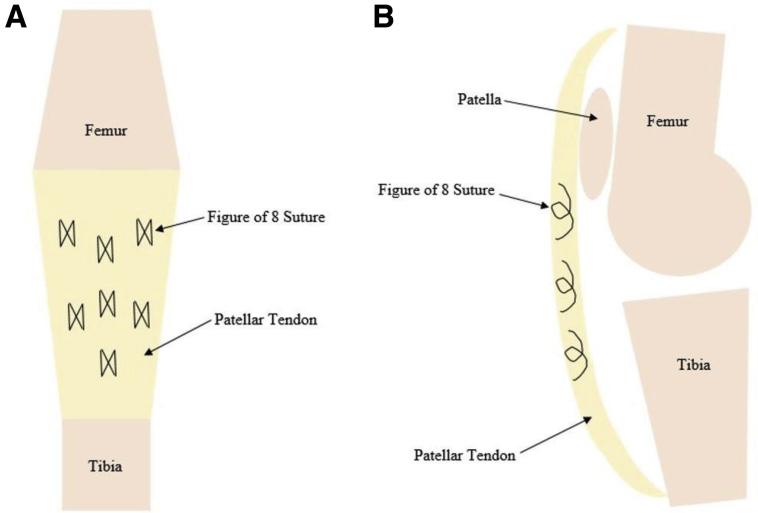
An anteroposterior (A) and lateral (B) schematic demonstrating the placement of the figure-of-eight sutures along the patellar tendon to complete the patellar tendon imbrication. Two figure-of-eight ORTHOCORD sutures (Mitek) are placed proximal to distal along both the medial and lateral aspect of the patellar tendon (4 in total). Then, 3 VICRYL figure-of-eight sutures (Ethicon) are placed centrally along the patellar tendon.
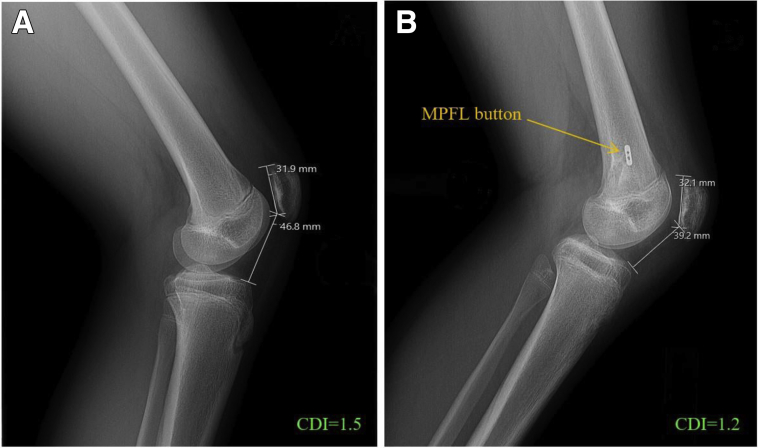
Lateral radiographs of a left knee demonstrating the measurement of the Caton–Deschamps index (CDI) preoperatively (A) and postoperatively (B) in a 15-year-old female patient with patella alta and patellar instability status post combined medial patellofemoral ligament reconstruction and patellar tendon imbrication. The CDI was 1.5 preoperatively and 1.2 postoperatively, showing a reduced patellar height.
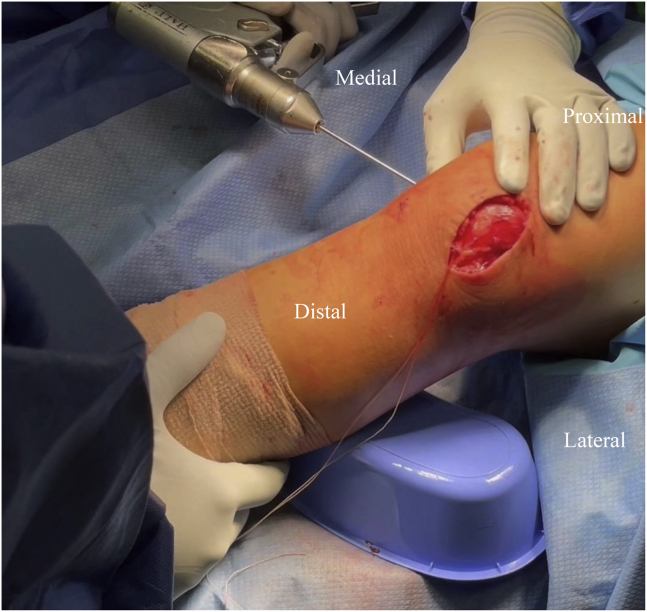
This image shows the patient placed in the supine position. On the left knee, a small incision is made just posterior to the medial epicondyle and a guide wire is drilled approximately 35 mm into the femur to establish the femoral tunnel.
This image shows the patient placed in the supine position. On the left knee, a spade-tip guidewire is drilled through the lateral femoral cortex. The skin is retracted to allow for palpation where the pin is coming through, ensuring there is not significant soft tissue under where the medial patellofemoral ligament button will sit.
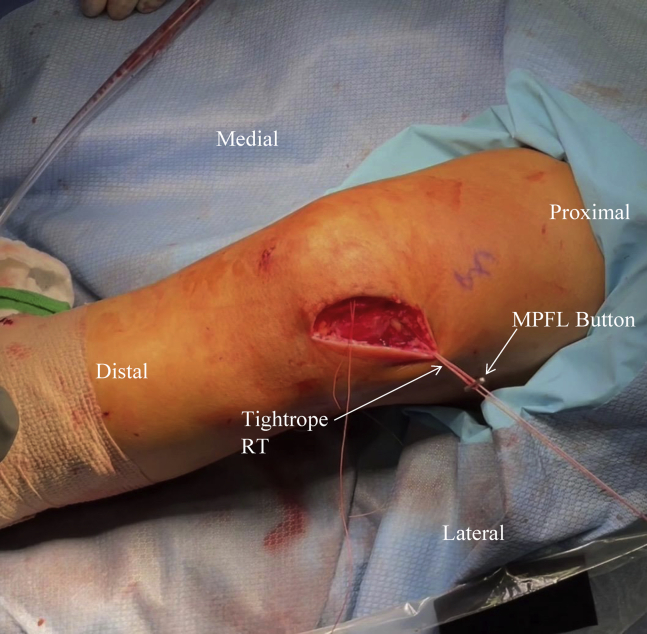
This image shows the patient placed in the supine position. On the left knee, the medial patellofemoral ligament (MPFL) is shown being secured into the femoral tunnel using the TightRope RT. The MPFL button will be fixated into the lateral aspect of the femur.
Similar articles
-
Efficacy of Transection-Free Patellar Tendon Imbrication Technique for the Correction of Patella Alta.Orthop J Sports Med. 2025 Apr 10;13(4):23259671251325752. doi: 10.1177/23259671251325752. eCollection 2025 Apr. Orthop J Sports Med. 2025. PMID: 40291632 Free PMC article.
-
Patellar Tendon Imbrication for Patella Alta.Arthrosc Tech. 2021 Dec 20;11(1):e7-e12. doi: 10.1016/j.eats.2021.08.029. eCollection 2022 Jan. Arthrosc Tech. 2021. PMID: 35127423 Free PMC article.
-
Patellar Tendon Shortening for Treatment of Patella Alta in Skeletally Immature Patients With Patellar Instability.Arthrosc Tech. 2021 Jul 20;10(8):e1979-e1984. doi: 10.1016/j.eats.2021.04.025. eCollection 2021 Aug. Arthrosc Tech. 2021. PMID: 34401243 Free PMC article.
-
What's up with patella alta?Curr Opin Pediatr. 2025 Feb 1;37(1):82-87. doi: 10.1097/MOP.0000000000001428. Epub 2024 Nov 29. Curr Opin Pediatr. 2025. PMID: 39699105 Review.
-
Radiographic and Clinical Outcomes After Tibial Tubercle Osteotomy for the Treatment of Patella Alta: A Systematic Review and Meta-analysis.Am J Sports Med. 2022 Jun;50(7):2042-2051. doi: 10.1177/03635465211012371. Epub 2021 May 26. Am J Sports Med. 2022. PMID: 34038256
Cited by
-
Distally Based Patella Tendon Shortening With Medial Patellotibial Ligament Reconstruction.Arthrosc Tech. 2024 Jun 27;13(10):103066. doi: 10.1016/j.eats.2024.103066. eCollection 2024 Oct. Arthrosc Tech. 2024. PMID: 39479038 Free PMC article.
-
Efficacy of Transection-Free Patellar Tendon Imbrication Technique for the Correction of Patella Alta.Orthop J Sports Med. 2025 Apr 10;13(4):23259671251325752. doi: 10.1177/23259671251325752. eCollection 2025 Apr. Orthop J Sports Med. 2025. PMID: 40291632 Free PMC article.
-
Proximal bone block with distal screw trajectory improves mechanical stability during distalization tibial tubercle osteotomy.Knee Surg Sports Traumatol Arthrosc. 2023 Oct;31(10):4239-4245. doi: 10.1007/s00167-023-07467-z. Epub 2023 Jun 10. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37300701
References
-
- Sanders T.L., Pareek A., Hewett T.E., Stuart M.J., Dahm D.L., Krych A.J. High rate of recurrent patellar dislocation in skeletally immature patients: A long-term population-based study. Knee Surg Sports Traumatol Arthrosc. 2018;26:1037–1043. - PubMed
-
- Biedert R.M. Patella alta: When to correct and impact on other anatomic risk factors for patellofemoral instability. Clin Sports Med. 2022;41:65–76. - PubMed
-
- Conry K.T., Cosgarea A.J., Tanaka M.J., Elias J.J. Influence of tibial tuberosity position and trochlear depth on patellar tracking in patellar instability: Variations with patella alta. Clin Biomech (Bristol, Avon) 2021;87 - PubMed
-
- Dejour H., Walch G., Nove-Josserand L., Guier C. Factors of patellar instability: An anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc. 1994;2:19–26. - PubMed
LinkOut - more resources
Full Text Sources
