

PD-1/PD-L1 immune-checkpoint blockade induces immune effector cell modulation in metastatic non-small cell lung cancer patients: A single-cell flow cytometry approach
- PMID: 36185285
- PMCID: PMC9515511
- DOI: 10.3389/fonc.2022.911579
PD-1/PD-L1 immune-checkpoint blockade induces immune effector cell modulation in metastatic non-small cell lung cancer patients: A single-cell flow cytometry approach
Abstract
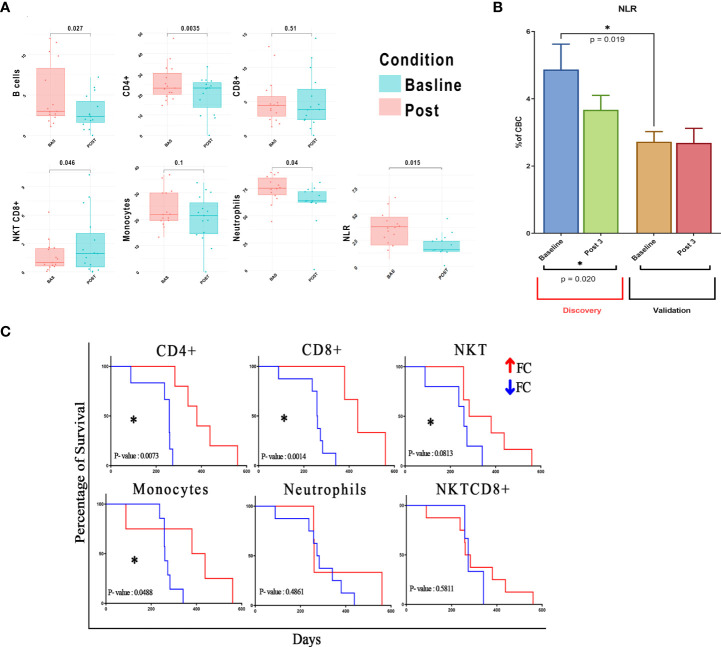
Peripheral immune-checkpoint blockade with mAbs to programmed cell death receptor-1 (PD-1) (either nivolumab or pembrolizumab) or PD-Ligand-1 (PD-L1) (atezolizumab, durvalumab, or avelumab) alone or in combination with doublet chemotherapy represents an expanding treatment strategy for metastatic non-small cell lung cancer (mNSCLC) patients. This strategy lays on the capability of these mAbs to rescue tumor-specific cytotoxic T lymphocytes (CTLs) inactivated throughout PD-1 binding to PD-L1/2 in the tumor sites. This inhibitory interactive pathway is a physiological mechanism of prevention against dangerous overreactions and autoimmunity in case of prolonged and/or repeated CTL response to the same antigen peptides. Therefore, we have carried out a retrospective bioinformatics analysis by single-cell flow cytometry to evaluate if PD-1/PD-L1-blocking mAbs modulate the expression of specific peripheral immune cell subsets, potentially correlated with autoimmunity triggering in 28 mNSCLC patients. We recorded a treatment-related decline in CD4+ T-cell and B-cell subsets and in the neutrophil-to-lymphocyte ratio coupled with an increase in natural killer T (NKT), CD8+PD1+ T cells, and eosinophils. Treatment-related increase in autoantibodies [mainly antinuclear antibodies (ANAs) and extractable nuclear antigen (ENA) antibodies] as well as the frequency of immune-related adverse events were associated with the deregulation of specific immune subpopulations (e.g., NKT cells). Correlative biological/clinical studies with deep immune monitoring are badly needed for a better characterization of the effects produced by PD-1/PD-L1 immune-checkpoint blockade.
Keywords: NKT; NSCL; bioinformatics; flow cytometry; immune checkpoint inhibitors.
Copyright © 2022 Fameli, Nardone, Shekarkar Azgomi, Bianco, Gandolfo, Oliva, Monoriti, Saladino, Falzea, Romeo, Calandruccio, Azzarello, Giannicola, Pirtoli, Giordano, Tassone, Tagliaferri, Cusi, Mutti, Botta and Correale.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials