

Hereditary hemochromatosis: Temporal trends, sociodemographic characteristics, and independent risk factor of hepatocellular cancer - nationwide population-based study
- PMID: 36185720
- PMCID: PMC9521447
- DOI: 10.4254/wjh.v14.i9.1804
Hereditary hemochromatosis: Temporal trends, sociodemographic characteristics, and independent risk factor of hepatocellular cancer - nationwide population-based study
Abstract
Background: Hereditary hemochromatosis (HH) has an increased risk of hepatocellular cancer (HCC) both due to genetic risks and iron overload as iron overload can be carcinogenic; HH impacts the increasing risk of HCC, not only through the development of cirrhosis but concerning hepatic iron deposition, which has been studied further recently.
Aim: To evaluate HH yearly trends, patient demographics, symptoms, comorbidities, and hospital outcomes. The secondary aim sheds light on the risk of iron overload for developing HCC in HH patients, independent of liver cirrhosis complications. The study investigated HH (without cirrhosis) as an independent risk factor for HCC.
Methods: We analyzed data from National Inpatient Sample (NIS) Database, the largest national inpatient data collection in the United States, and selected HH and HCC cohorts. HH was first defined in 2011 International Classification of Disease - 9th edition (ICD-9) as a separate diagnosis; the HH cohort is extracted from January 2011 to December 2019 using 275.01 (ICD-9) and E83.110 (ICD-10) diagnosis codes of HH. Patients were excluded from the HH cohort if they had a primary or secondary diagnostic code of cirrhosis (alcoholic, non-alcoholic, and biliary), viral hepatitis, alcoholic liver disease, non-alcoholic fatty liver disease (NAFLD), and non-alcoholic steatohepatitis (NASH). We removed these patients from the HH cohort to rule out bias or ICD-10 diagnostic errors. The HCC cohort is selected from January 2011 to December 2019 using the ICD-9 and ICD-10 codes of HCC. We selected a non-HCC cohort with the 1:1 fixed ratio nearest neighbor (greedy) propensity score method using the patients' age, gender, and race. We performed multivariate analysis for the risk factors of HCC in the HCC and non-HCC matched cohort. We further analyzed HH without cirrhosis (removing HH patients with a diagnosis of cirrhosis) as an independent risk factor of HCC after adjusting all known risk factors of HCC in the multivariate model.
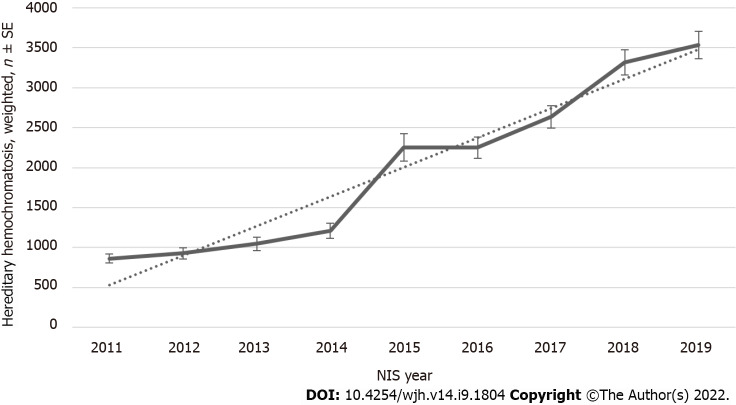
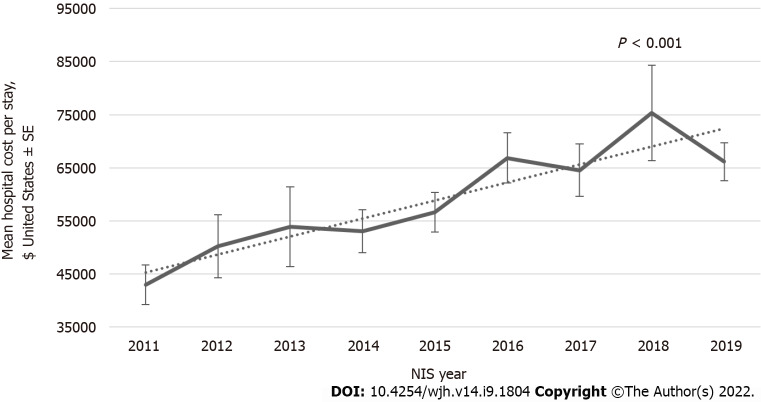
Results: During the 2011-2019 period, a total of 18031 hospitalizations with a primary or secondary diagnosis of HH (excluding liver diseases) were recorded in the NIS database. We analyzed different patients' characteristics, and we found increments in inpatient population trend with a Ptrend < 0.001 and total hospital cost of care trend from $42957 in 2011 to $66152 in 2019 with a Ptrend < 0.001 despite no change in Length of Stay over the last decade. The multivariate analyses showed that HH without cirrhosis (aOR, 28.8; 95%CI, 10.4-80.1; P < 0.0001), biliary cirrhosis (aOR, 19.3; 95%CI, 13.4-27.6; P < 0.0001), non-alcoholic cirrhosis (aOR, 17.4; 95%CI, 16.5-18.4; P < 0.0001), alcoholic cirrhosis (aOR, 16.9; 95%CI, 15.9-17.9; P < 0.0001), hepatitis B (aOR, 12.1; 95%CI, 10.85-13.60; P < 0.0001), hepatitis C (aOR, 8.58; 95%CI, 8.20-8.98; P < 0.0001), Wilson disease (aOR, 4.27; 95%CI, 1.18-15.41; P < 0.0001), NAFLD or NASH (aOR, 2.96; 95%CI, 2.73-3.20; P < 0.0001), alpha1-antitrypsin deficiency (aOR, 2.10; 95%CI, 1.21-3.64; P < 0.0001), diabetes mellitus without chronic complications (aOR, 1.17; 95%CI, 1.13-1.21; P < 0.0001), and blood transfusion (aOR, 1.80; 95%CI, 1.69-1.92; P < 0.0001) are independent risk factor for liver cancer.
Conclusion: Our study showed an increasing trend of in-hospital admissions of HH patients in the last decade. These trends were likely related to advances in diagnostic approach, which can lead to increased hospital utilization and cost increments. Still, the length of stay remained the same, likely due to a big part of management being done in outpatient settings. Another vital part of our study is the significant result that HH without cirrhosis is an independent risk factor for HCC with adjusting all known risk factors. More prospective and retrospective large studies are needed to re-evaluate the HH independent risk in developing HCC.
Keywords: Alpha1-antitrypsin deficiency; Big data; Blood transfusion; Demographics; Diabetes mellitus; Epidemiology; Hepatitis; Hepatocellular carcinoma, cirrhosis; Hereditary hemochromatosis; Hospitalization; Nonalcoholic fatty liver disease; Nonalcoholic steatohepatitis; Wilson disease.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare no conflict of interests for this article.
Figures

References
-
- Porter JL, Rawla P. Hemochromatosis. 2022 Jun 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
-
- Golfeyz S, Lewis S, Weisberg IS. Hemochromatosis: pathophysiology, evaluation, and management of hepatic iron overload with a focus on MRI. Expert Rev Gastroenterol Hepatol. 2018;12:767–778. - PubMed
LinkOut - more resources
Full Text Sources
