

Analgesic Efficacy of Adjuvant Medications in the Pediatric Caudal Block for Infraumbilical Surgery: A Network Meta-Analysis of Randomized Controlled Trials
- PMID: 36185831
- PMCID: PMC9521396
- DOI: 10.7759/cureus.28582
Analgesic Efficacy of Adjuvant Medications in the Pediatric Caudal Block for Infraumbilical Surgery: A Network Meta-Analysis of Randomized Controlled Trials
Abstract
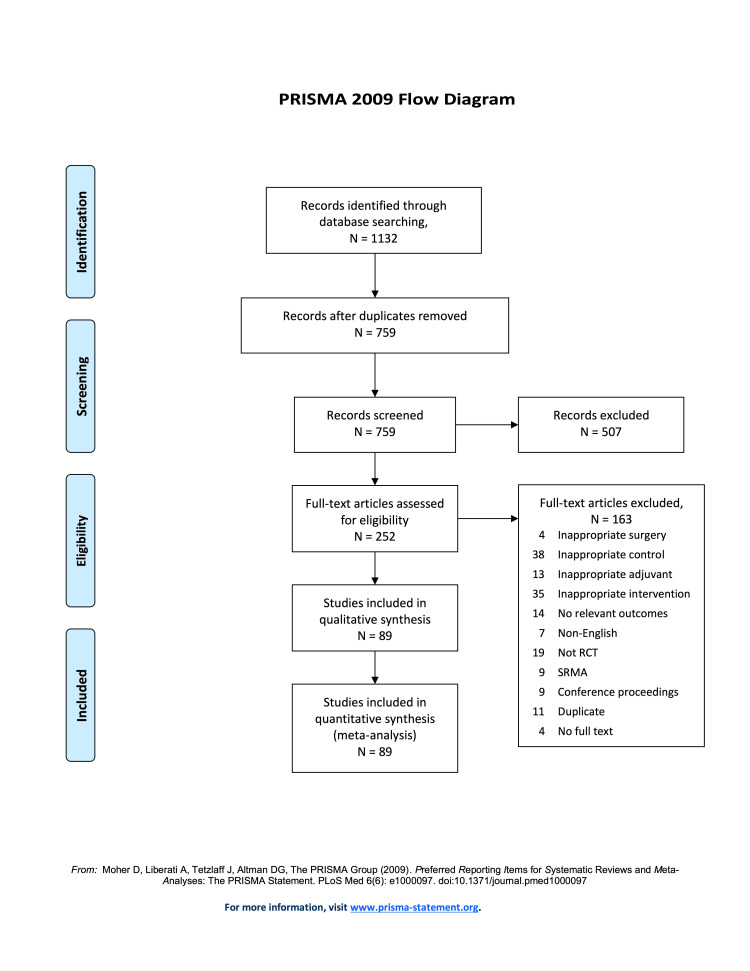
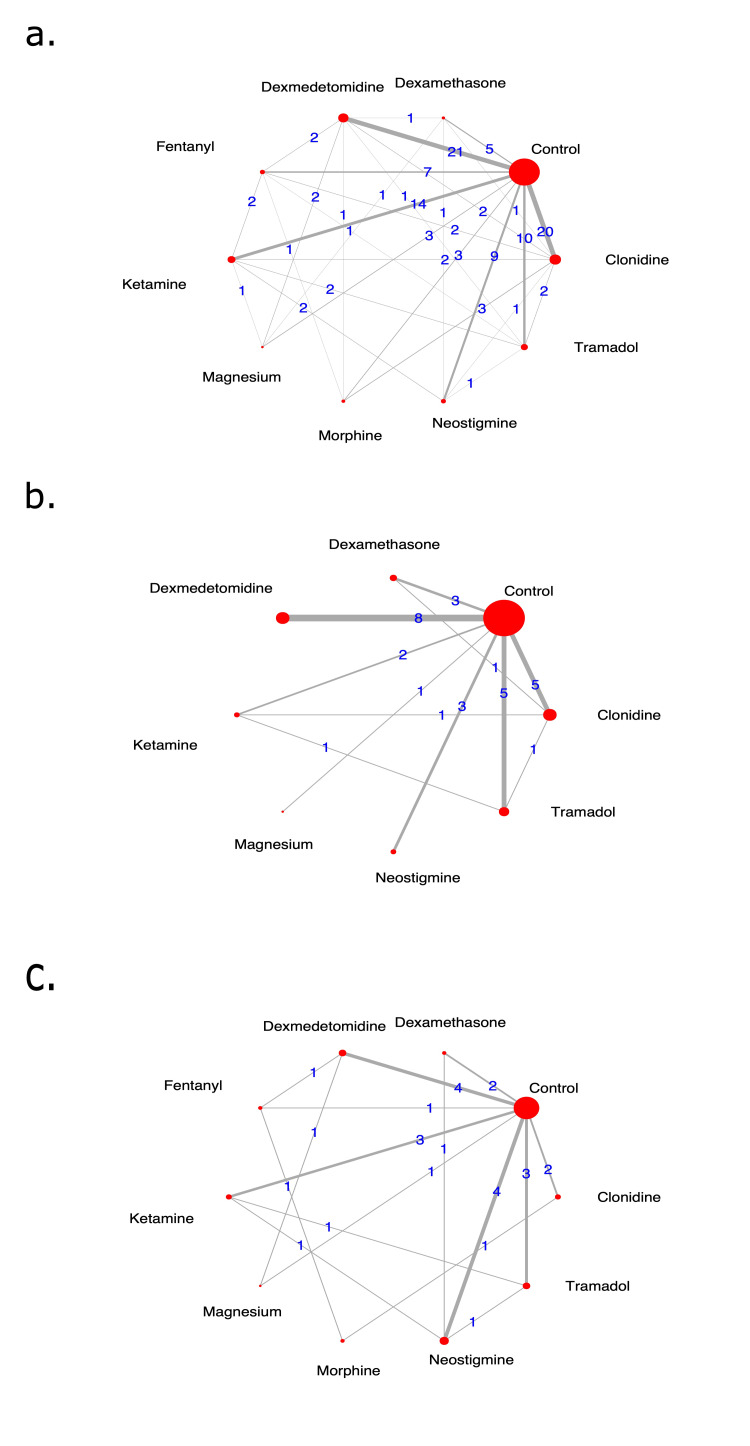
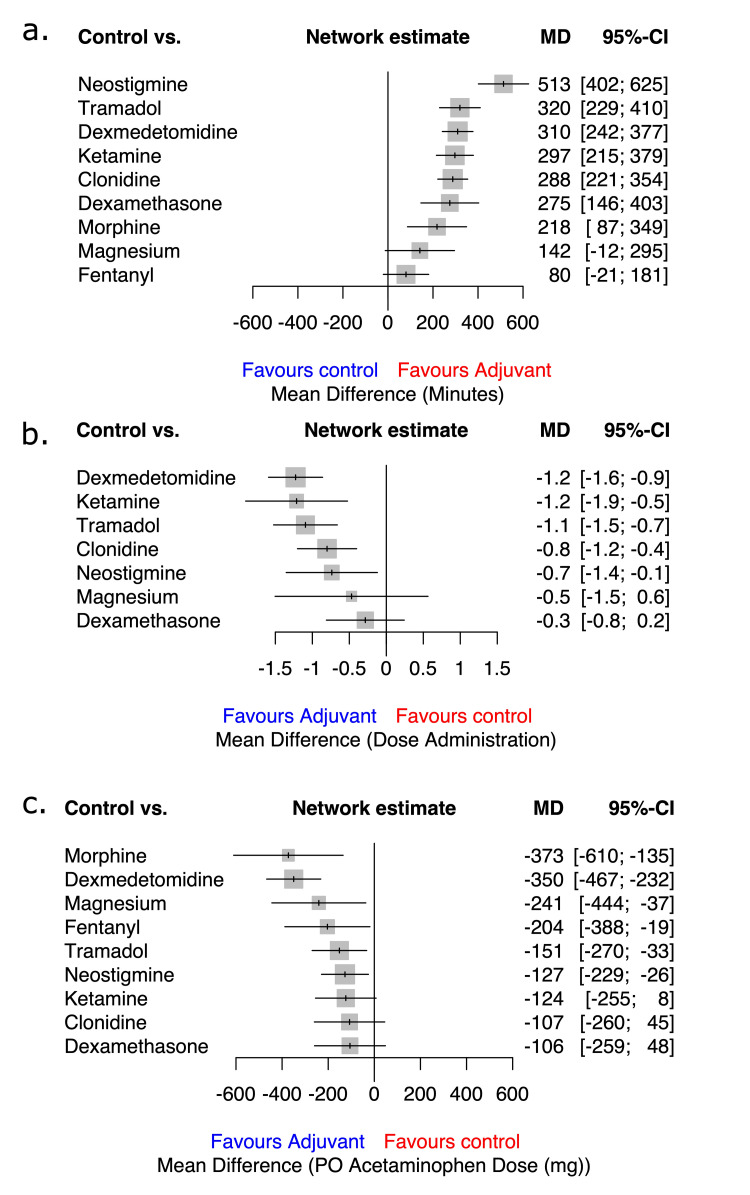
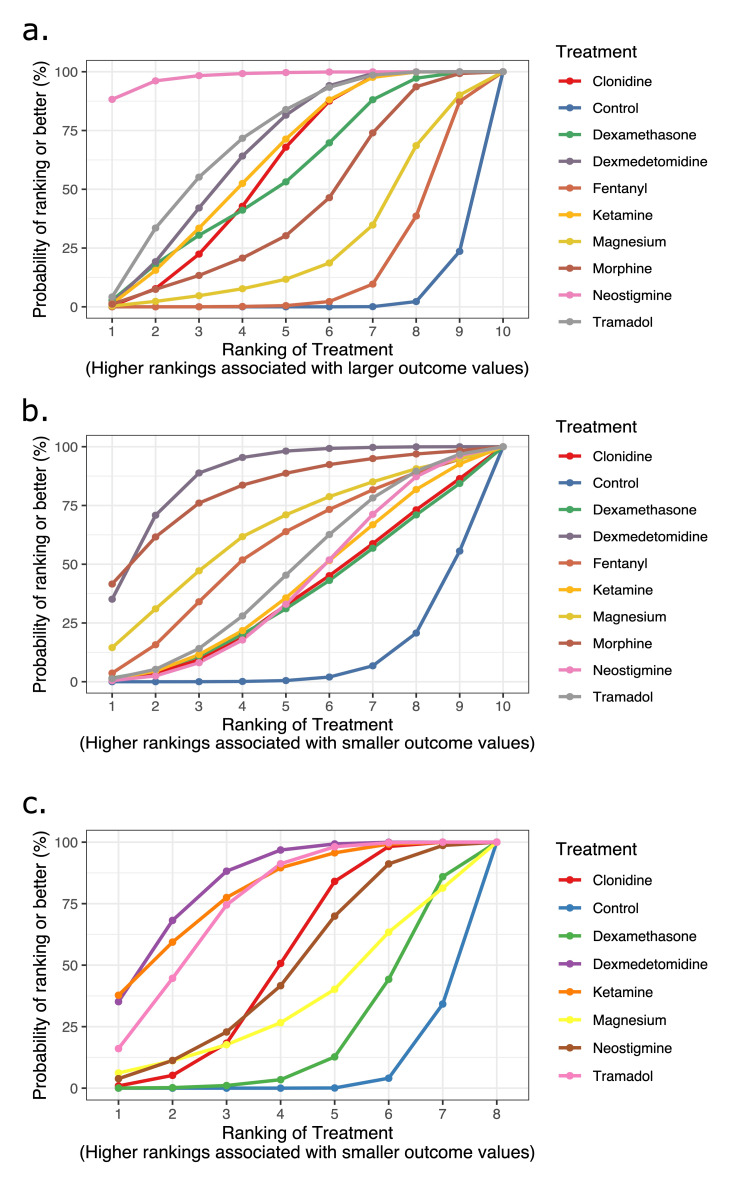
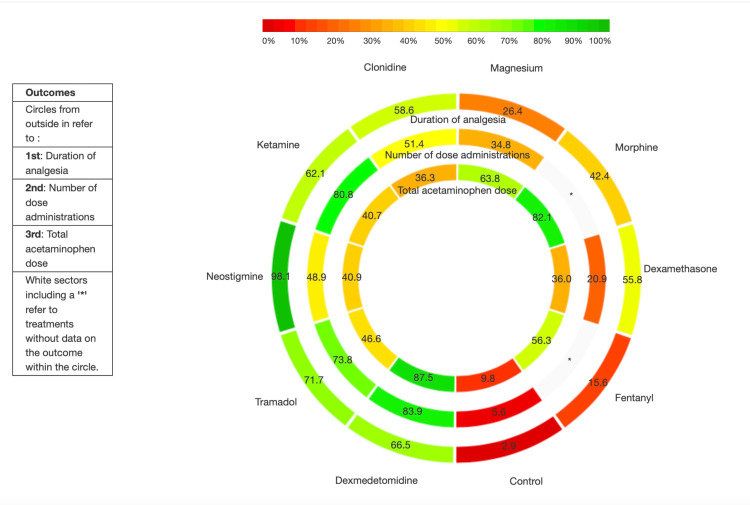
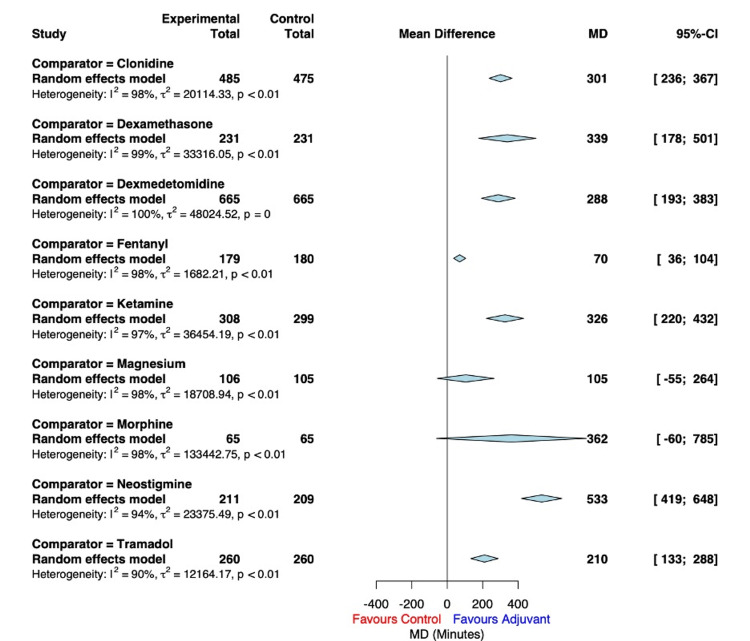
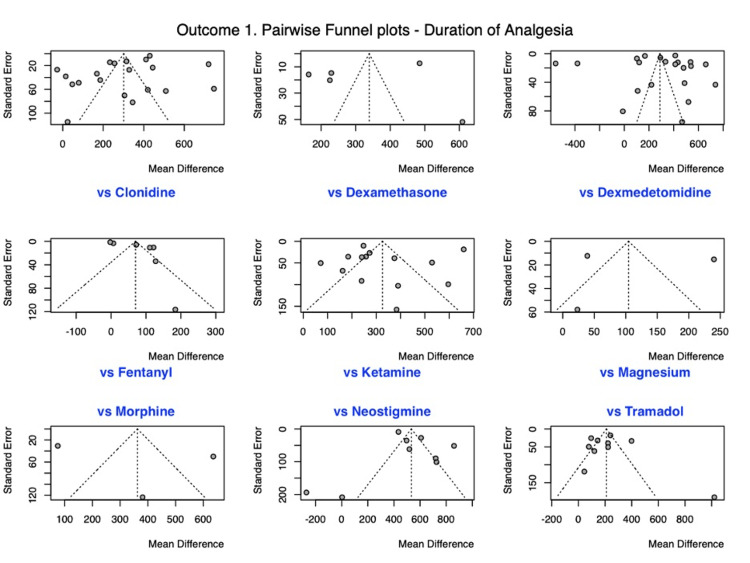
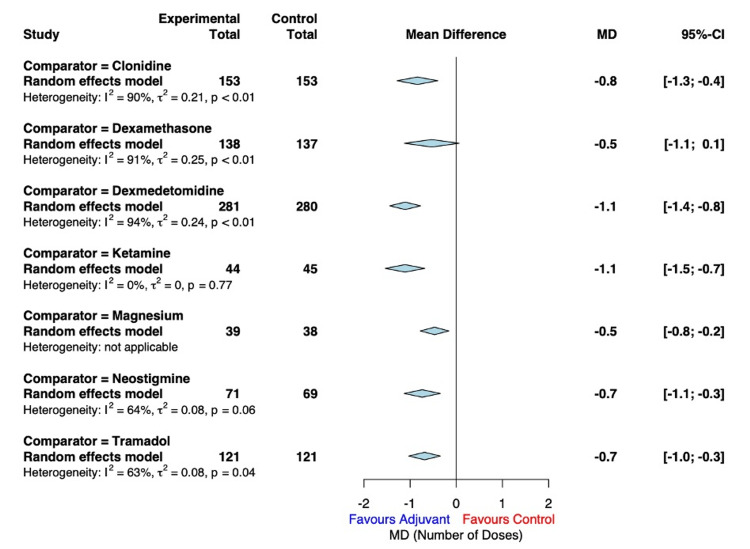
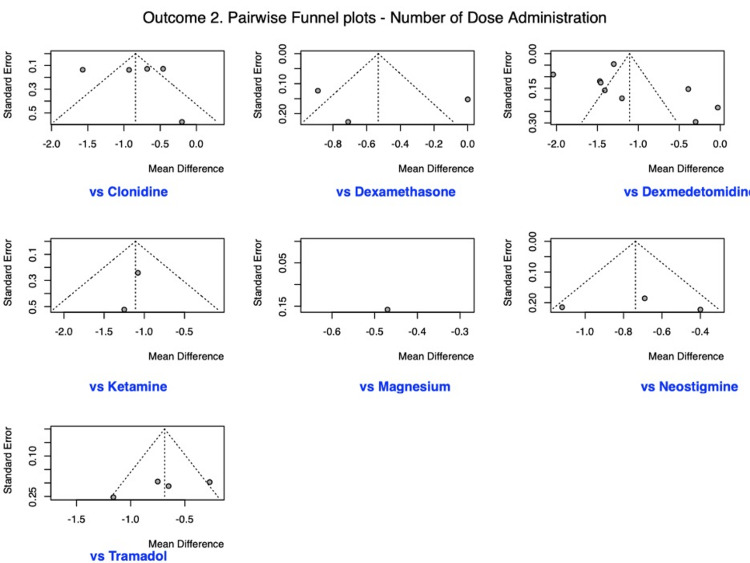
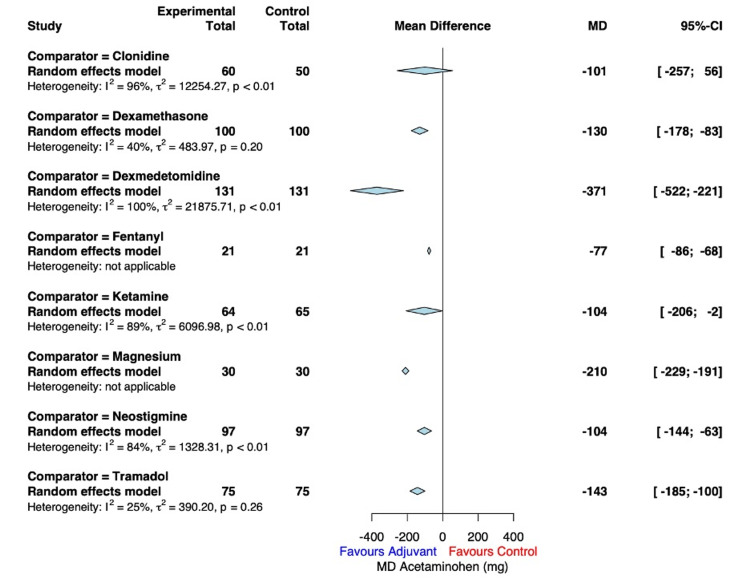
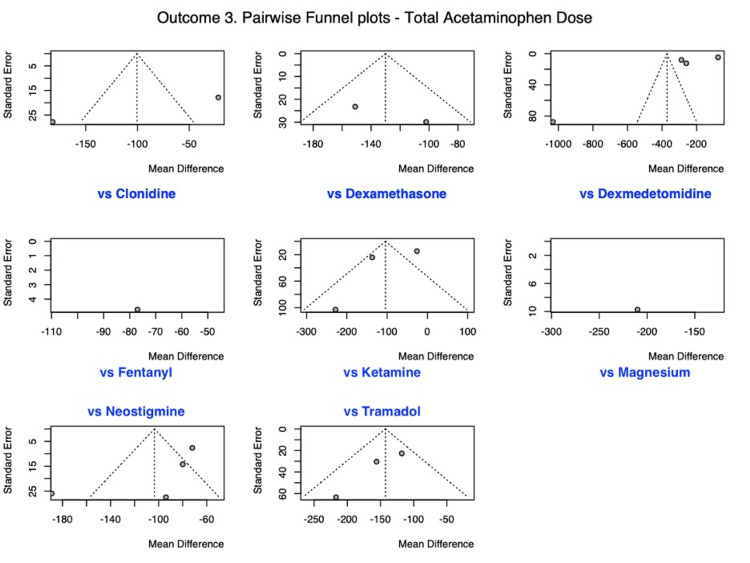
Various adjuvants are added to local anesthetics in caudal block to improve analgesia. The comparative analgesic effectiveness and relative rankings of these adjuvants are unknown. This network meta-analysis (NMA) sought to evaluate the comparative analgesic efficacy and relative ranking of caudal adjuvants added to local anesthetics (versus local anesthetics alone) in pediatric infra-umbilical surgery. We searched the United States National Library of Medicine database (MEDLINE), PubMed, and Excerpta Medica database (Embase) for randomized controlled trials (RCTs) comparing caudal adjuvants (clonidine, dexmedetomidine, ketamine, magnesium, morphine, fentanyl, tramadol, dexamethasone, and neostigmine) among themselves, or to no adjuvant (control). We performed a frequentist NMA and employed Cochrane's 'Risk of Bias' tool to evaluate study quality. We chose the duration of analgesia (defined as 'the time from caudal injection to the time of rescue analgesia') as our primary outcome. We also assessed the number of analgesic dose administrations and total dose of acetaminophen within 24 h. The duration of analgesia [87 randomized control trials (RCTs), 5285 patients] was most prolonged by neostigmine [mean difference: 513 min, (95% confidence interval, CI: 402, 625)]. Dexmedetomidine reduced the frequency of analgesic dose administrations within 24 h [29 RCTs, 1765 patients; -1.2 dose (95% CI: -1.6, -0.9)] and the total dose of acetaminophen within 24 h [18 RCTs, 1156 patients; -350 mg (95% CI: -467, -232)] the most. Among caudal adjuvants, neostigmine (moderate certainty), tramadol (low certainty), and dexmedetomidine (low certainty) prolonged the duration of analgesia the most. Dexmedetomidine also reduced the analgesic frequency and consumption more than other caudal adjuvants (moderate certainty).
Keywords: adjuvant; caudal; local anesthesia; network meta-analysis; pain; pediatric; post-operative.
Copyright © 2022, Shah et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparison of adjuvant pharmaceuticals for caudal block in pediatric lower abdominal and urological surgeries: A network meta-analysis.J Clin Anesth. 2022 Oct;81:110907. doi: 10.1016/j.jclinane.2022.110907. Epub 2022 Jun 18. J Clin Anesth. 2022. PMID: 35728381 Review.
-
Efficacy and safety of caudal dexmedetomidine in pediatric infra-umbilical surgery: a meta-analysis and trial-sequential analysis of randomized controlled trials.Reg Anesth Pain Med. 2021 May;46(5):422-432. doi: 10.1136/rapm-2020-102024. Epub 2021 Jan 15. Reg Anesth Pain Med. 2021. PMID: 33452203 Review.
-
Clonidine as an Additive to Local Anesthetics in Caudal Block for Postoperative Analgesia in Pediatric Surgery: A Systematic Review and Meta-Analysis.Front Med (Lausanne). 2021 Sep 14;8:723191. doi: 10.3389/fmed.2021.723191. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34595191 Free PMC article.
-
Nonopioid (Dexmedetomidine, Dexamethasone, Magnesium) Adjuvant to Ropivacaine Caudal Anesthesia in Pediatric Patients Undergoing Infraumbilical Surgeries: A Comparative Study.Anesth Essays Res. 2017 Jul-Sep;11(3):636-641. doi: 10.4103/0259-1162.206853. Anesth Essays Res. 2017. PMID: 28928562 Free PMC article.
-
Dexmedetomidine as an adjuvant to bupivacaine in caudal analgesia in children.Anesth Essays Res. 2016 May-Aug;10(2):227-32. doi: 10.4103/0259-1162.174468. Anesth Essays Res. 2016. PMID: 27212752 Free PMC article.
Cited by
-
Evaluating Caudal Block Enhancements in Pediatric Circumcision: Do Additional Analgesics Make a Difference?Med Sci Monit. 2023 Oct 31;29:e942557. doi: 10.12659/MSM.942557. Med Sci Monit. 2023. PMID: 37904341 Free PMC article. Clinical Trial.
References
-
- Are caudal blocks for pain control safe in children? an analysis of 18,650 caudal blocks from the Pediatric Regional Anesthesia Network (PRAN) database. Suresh S, Long J, Birmingham PK, De Oliveira GS Jr. Anesth Analg. 2015;120:151–156. - PubMed
-
- Epidemiology and morbidity of regional anesthesia in children: a follow-up one-year prospective survey of the French-Language Society of Paediatric Anaesthesiologists (ADARPEF) Ecoffey C, Lacroix F, Giaufré E, Orliaguet G, Courrèges P. Paediatr Anaesth. 2010;20:1061–1069. - PubMed
-
- The European Society of Regional Anaesthesia and Pain Therapy/American Society of Regional Anesthesia and Pain Medicine Recommendations on Local Anesthetics and Adjuvants Dosage in Pediatric Regional Anesthesia. Suresh S, Ecoffey C, Bosenberg A, et al. Reg Anesth Pain Med. 2018;43:211–216. - PubMed
-
- Caudal and epidural blocks in infants and small children: historical perspective and ultrasound-guided approaches. Kil HK. https://pubmed.ncbi.nlm.nih.gov/30086609/ Kor J Anesthesiol. 2018;71:430–439. - PMC - PubMed
-
- Pediatric Regional Anesthesia Network (PRAN): a multi-institutional study of the use and incidence of complications of pediatric regional anesthesia. Polaner DM, Taenzer AH, Walker BJ, et al. Anesth Analg. 2012;115:1353–1364. - PubMed
Publication types
LinkOut - more resources
Full Text Sources