

Disorders of Arousal and timing of the first period of slow wave sleep: Clinical and forensic implications
- PMID: 36187082
- PMCID: PMC9520070
- DOI: 10.1016/j.sleepx.2022.100057
Disorders of Arousal and timing of the first period of slow wave sleep: Clinical and forensic implications
Abstract
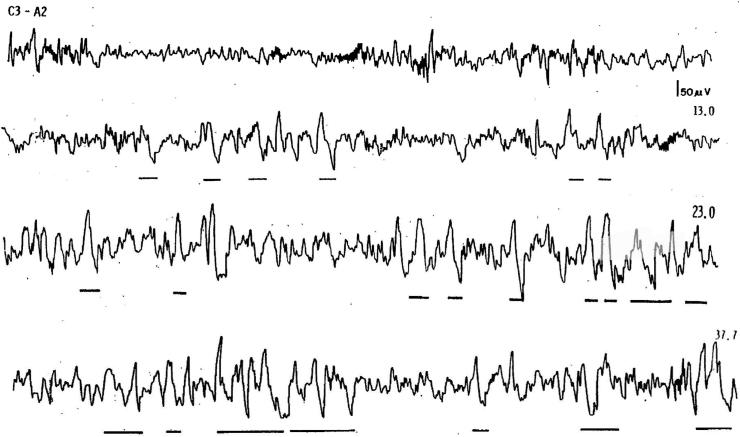
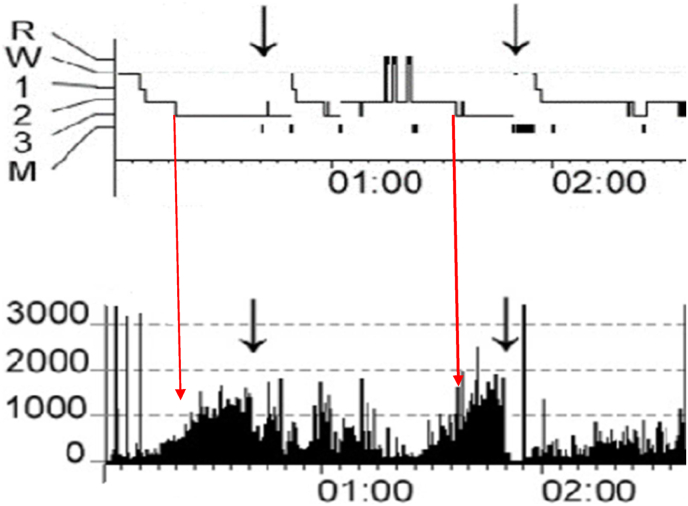
The timing of first period of slow wave sleep (SWS) is often used as a proxy for determining if and when Disorders of Arousal (DOA) such as sleepwalking are likely to occur or did occur in the past. In criminal cases employing a "sleepwalking defense" the prosecution may argue that nocturnal violence or sexually aggressive behavior occurred too early in the sleep period to be associated with SWS. Expert witness opinion on the expected latency to SWS (LSWS) has varied from minutes after sleep onset to ≥60 min. A search of PubMed was conducted for LSWS and for any reports of DOAs occurring from stage N2. A total of 21 studies reported LSWS in normal controls, clinically diagnosed sleepwalkers, in otherwise normal sleepers following different types of sleep deprivation and due to the effects of alcohol. Five studies reported episodes of DOA from N2 sleep. The shortest mean LSWS of 6.4 min was found with a combination of total sleep deprivation and alcohol. In a group of normal research subjects, a LSWS mean of 10.7 min was noted. LSWS in DOA patients occurred as early as a mean of 12.4 min. Two sleep studies performed on Kenneth Parks, acquitted of the murder of his mother-in-law by a sleepwalking defense, reported LSWSs of 9.7 and 10 min. Sleep deprivation but not alcohol was found to decrease LSWS significantly. Expert opinions on LSWS should be based on scientific peer reviewed publications documenting empirical sleep evidence and can be much shorter than is generally reported.
Keywords: Alcohol; DOA, Disorder of Arousal; Disorder of arousal; Forensic evaluation; Kenneth parks; LSWS, Latency to Slow Wave Sleep; Latency to slow wave sleep; N3; NREM, Non-Rapid Eye Movement Sleep; SWS, Slow Wave Sleep; Sexual behavior in sleep; Sleep deprivation; Sleepwalking defense; Sleepwalking violence; Slow wave sleep.
© 2022 The Author.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Academy_of_Sleep_Medicine A. 2014. International classificatin of sleep disorders version 3: diagnostic and coding manual.
-
- Berry R.B.Q.S., Abreu A.R., Bibbs M.L., DelRosso L., Harding S.M., Mao M., Plante D.T., Pressman M.R., Troester M.M. 6 ed. American Academy of Sleep Medicine.; Darien, IL: 2020. Vaughn the AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications.
-
- Pressman Mark., Ph.D. American Psychological Association; Washington, D.c.: 2018. Sleepwalking, Criminal behavior and reliable scientific evidence: a guide for experts.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
