

Use of a non-endoscopic immunocytological device (Cytosponge™) for post chemoradiotherapy surveillance in patients with oesophageal cancer in the UK (CYTOFLOC): A multicentre feasibility study
- PMID: 36187722
- PMCID: PMC9519482
- DOI: 10.1016/j.eclinm.2022.101664
Use of a non-endoscopic immunocytological device (Cytosponge™) for post chemoradiotherapy surveillance in patients with oesophageal cancer in the UK (CYTOFLOC): A multicentre feasibility study
Abstract
Background: Effective surveillance strategies are required for patients diagnosed with oesophageal squamous cell carcinoma (OSCC) or adenocarcinoma (OAC) for whom chemoradiotherapy (CRT) is used as a potentially-curative, organ-sparing, alternative to surgery. In this study, we evaluated the safety, acceptability and tolerability of a non-endoscopic immunocytological device (the Cytosponge™) to assess treatment response following CRT.
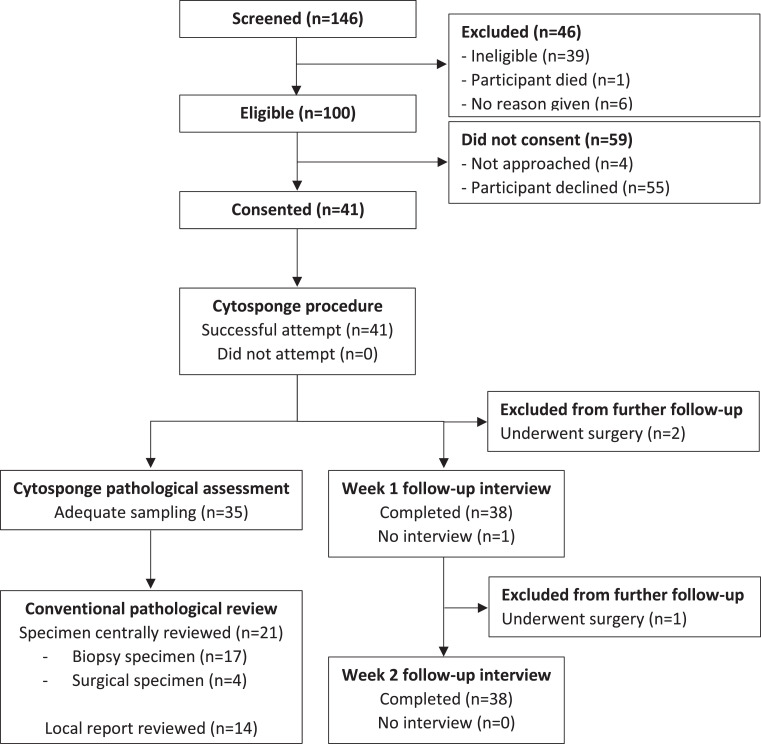
Methods: This multicentre, single-arm feasibility trial took place in 10 tertiary cancer centres in the UK. Patients aged at least 16 years diagnosed with OSCC or OAC, and who were within 4-16 weeks of completing definitive or neo-adjuvant CRT, were included. Participants were required to have a Mellow-Pinkas dysphagia score of 0-2 and be able to swallow tablets. All patients underwent a single Cytosponge™ assessment in addition to standard of care (which included post-treatment endoscopic evaluation with biopsy for patients undergoing definitive CRT; surgery for those who received neo-adjuvant CRT). The primary outcome was the proportion of consented, evaluable patients who successfully underwent Cytosponge™ assessment. Secondary and tertiary outcomes included safety, study consent rate, acceptance rate, the suitability of obtained samples for biomarker analysis, and the comparative efficacy of Cytosponge™ to standard histology (endoscopy and biopsy or post-resection specimen) in assessing for residual disease. The trial is registered with ClinicalTrials.gov, NCT03529669.
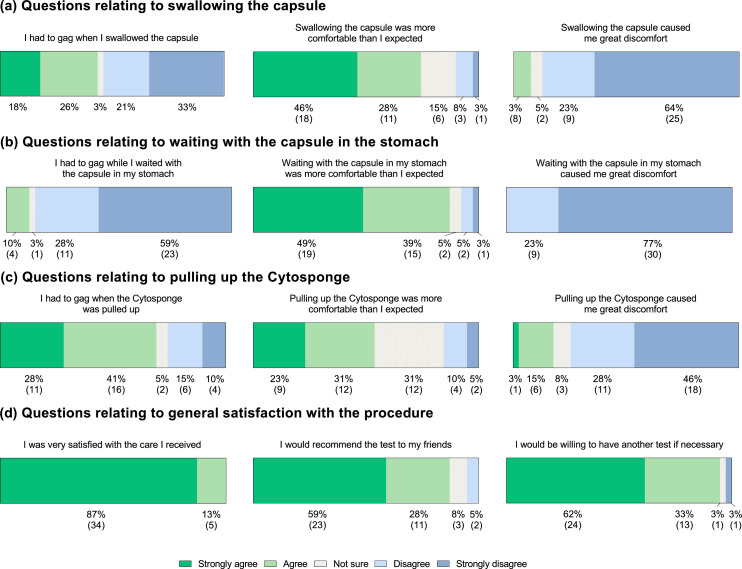
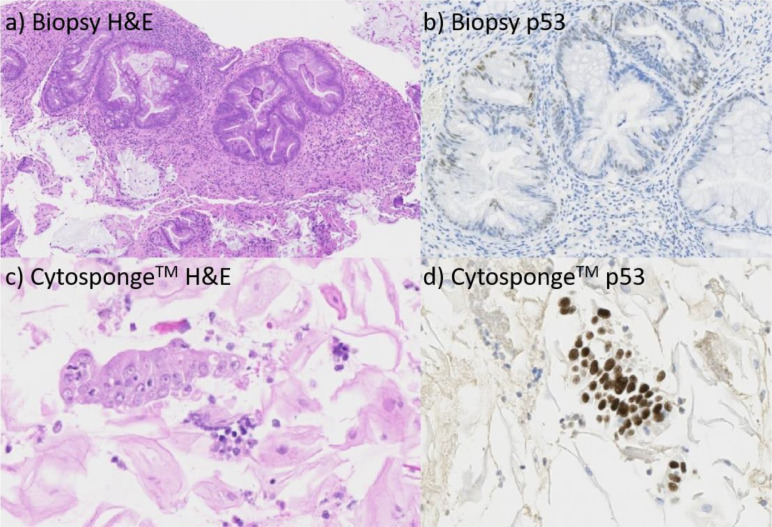
Findings: Between 18th April 2018 and 16th January 2020, 41 (42.7%; 95% confidence interval (CI) 32.7-53.2) of 96 potentially eligible patients consented to participate. Thirty-nine (95.1%, 95% CI 83.5-99.4) successfully carried out the Cytosponge™ procedure. Of these, 37 (95%) would be prepared to repeat the procedure. There were only two grade 1 adverse events attributed to use of the Cytosponge™. Thirty-five (90%) of the completed Cytosponge™ samples were suitable for biomarker analysis; 29 (83%) of these were concordant with endoscopic biopsies, three (9%) had findings suggestive of residual cancer on Cytosponge™ not found on endoscopic biopsies, and three (9%) had residual cancer on endoscopic biopsies not detected by Cytosponge™.
Interpretation: Use of the CytospongeTM is safe, tolerable, and acceptable for the assessment of treatment response following CRT in OAC and OSCC. Further evaluation of Cytosponge™ in this setting is warranted.
Funding: Cancer Research UK, National Institute for Health Research, Medical Research Council.
Keywords: Chemoradiation; Cytosponge; Oesophageal Cancer; Radiation; Surveillance.
© 2022 Published by Elsevier Ltd.
Conflict of interest statement
The Cytosponge™ technology including the device and TFF3 biomarker has been licensed by the MRC to Covidien (now Medtronic). R.C.F. and M.O.D. are named on patents related to this test. R.C.F. and M.O.D. are shareholders and consultants for Cyted, an early detection company. All other authors declare no competing interests.
Figures
References
-
- Kamangar F, Nasrollahzadeh D, Safiri S, et al. The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5:582–597. - PMC - PubMed
-
- Stahl M, Stuschke M, Lehmann N, et al. Chemoradiation with and without surgery in patients with locally advanced squamous cell carcinoma of the esophagus. J. Clin. Oncol. 2005;23:2310–2317. - PubMed
-
- Bedenne L, Michel P, Bouche O, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J. Clin. Oncol. 2007;25:1160–1168. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
