

Unilateral Biportal Endoscopic Discectomy versus Microendoscopic Discectomy for the Treatment of Lumbar Spinal Stenosis: A Systematic Review and Meta-Analysis
- PMID: 36188105
- PMCID: PMC9519329
- DOI: 10.1155/2022/7667463
Unilateral Biportal Endoscopic Discectomy versus Microendoscopic Discectomy for the Treatment of Lumbar Spinal Stenosis: A Systematic Review and Meta-Analysis
Abstract
Objective: In minimally invasive spinal surgery, the treatment of lumbar spinal stenosis with microendoscopic discectomy (MED) or unilateral biportal endoscopic discectomy (UBED) shows effective results, but which is more effective is controversial. Our study aimed to evaluate the efficacy and safety of UBED versus MED in the treatment of lumbar spinal stenosis by a systematic review and meta-analysis, so as to provide reference for the promotion of UBED in clinical practice.
Methods: The multiple databases like PubMed, EMBASE, Web of Science, Cochrane Library, Chinese National Knowledge Databases, Chinese BioMedical Database, and Wanfang Database were used to search for the relevant studies. Review Manager 5.4 was adopted to estimate the effects of the results among selected articles. Odds ratio (OR) and mean difference (MD) with 95% confidence intervals (CIs) were used to estimate the overall pooled effect. Subgroup analysis, forest plots, funnel plots and Egger's test for the articles included were also conducted.
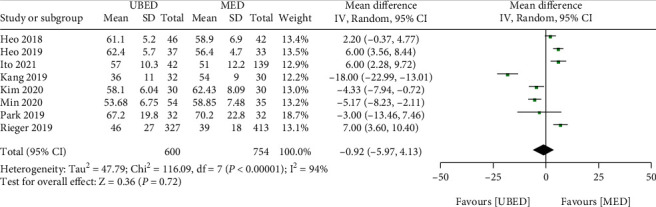
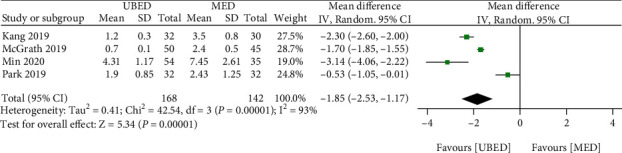
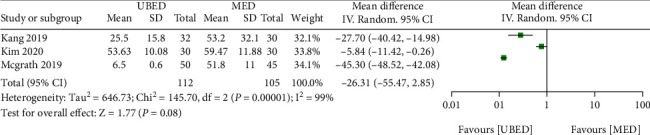
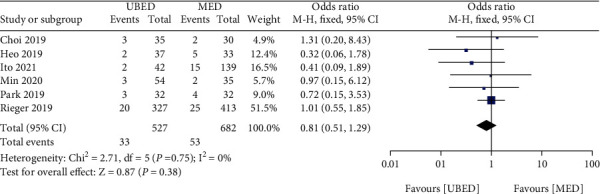
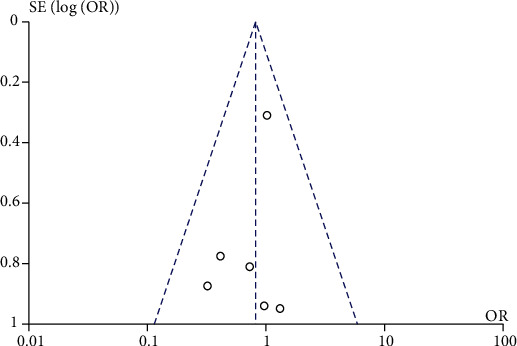
Results: Three randomized clinical trials and seven cohort studies were finally retrieved, these studies included 685 and 829 patients in the UBED and MED groups, respectively. There were no differences in terms of operation time (MD = -0.92, P =0.72), estimated blood loss (MD = -26.31, P =0.08), complications (MD =0.81, P =0.38) and Oswestry Disability Index (ODI) score (P >0.05 in four subgroup) between the two groups. The visual analog scale (VAS) score of back pain in the UBED group was better than MED group only at 6 months (MD = -0.23, P =0.006) after operation, the VAS score of leg pain in the UBED group was better than that of MED group at 3 mouths (MD = -0.22, P =0.002) and 6 months (MD = -0.24, P =0.006) after operation, the UBED group had a less postoperative length of stay than the MED group (MD = -1.85, P <0.001). The bias analysis showed that there was no potential publication bias in the included literature.
Conclusion: This study showed that compared with MED, UBED has the advantages of short hospital stay and good short-term curative effect, but there is no significant difference in long-term efficacy and safety, they can be replaced by each other in clinical application.
Copyright © 2022 Yufei Niu et al.
Conflict of interest statement
The author(s) declare(s) that they have no conflicts of interest.
Figures




Similar articles
-
Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: a meta-analysis.Int Orthop. 2019 Apr;43(4):923-937. doi: 10.1007/s00264-018-4253-8. Epub 2018 Dec 13. Int Orthop. 2019. PMID: 30547214
-
Unilateral biportal endoscopic discectomy versus microdiscectomy for lumbar disc herniation: a systematic review and meta-analysis.Eur Spine J. 2024 Jun;33(6):2139-2153. doi: 10.1007/s00586-023-08116-2. Epub 2024 Feb 22. Eur Spine J. 2024. PMID: 38388729
-
Unilateral Biportal Endoscopic Discectomy versus Percutaneous Endoscopic Lumbar Discectomy for Lumbar Disc Herniation: A Systematic Review and Meta-analysis.World Neurosurg. 2023 May;173:e509-e520. doi: 10.1016/j.wneu.2023.02.087. Epub 2023 Feb 24. World Neurosurg. 2023. PMID: 36841538
-
[Comparative analysis of unilateral biportal endoscopic discectomy, percutaneous endoscopic lumbar discectomy, and fenestration discectomy in treatment of lumbar disc herniation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022 Oct 15;36(10):1200-1206. doi: 10.7507/1002-1892.202205129. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022. PMID: 36310455 Free PMC article. Chinese.
-
Comparison of percutaneous endoscopic transforaminal discectomy, microendoscopic discectomy, and microdiscectomy for symptomatic lumbar disc herniation: minimum 2-year follow-up results.J Neurosurg Spine. 2018 Mar;28(3):317-325. doi: 10.3171/2017.6.SPINE172. Epub 2018 Jan 5. J Neurosurg Spine. 2018. PMID: 29303471
Cited by
-
Unilateral biportal endoscopic versus microscopic discectomy in degenerative lumbar spinal stenosis: A prospective cohort study.Medicine (Baltimore). 2025 May 23;104(21):e42594. doi: 10.1097/MD.0000000000042594. Medicine (Baltimore). 2025. PMID: 40419907 Free PMC article. Clinical Trial.
-
Surgical Outcomes of Full-Endoscopic Degenerative Lumbar Lateral Recess Stenosis Decompression Through an Interlaminar Approach.Orthop Surg. 2025 Apr;17(4):1181-1189. doi: 10.1111/os.14376. Epub 2025 Feb 24. Orthop Surg. 2025. PMID: 39993943 Free PMC article.
References
-
- Jensen R. K., Jensen T. S., Koes B., Hartvigsen J. Prevalence of lumbar spinal stenosis in general and clinical populations: a systematic review and meta-analysis. European Spine Journal . 2020;29(17):252–272. - PubMed
-
- Bing W., Lu G., Liu W. Analysis of the causes of intraoperative conversion to open surgery for full endoscopic interlaminar disectomy. Chinese Journal of Spine & Spinal Cord . 2011;14(8):123–128.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
