

Comparison of Real-World Dose and Consumption for Two Extended Half-Life Recombinant Factor VIII Products for the Treatment of Hemophilia A in the United States
- PMID: 36188439
- PMCID: PMC9518681
- DOI: 10.2147/JBM.S359510
Comparison of Real-World Dose and Consumption for Two Extended Half-Life Recombinant Factor VIII Products for the Treatment of Hemophilia A in the United States
Abstract
Background: US patients with hemophilia A can receive prophylaxis with extended half-life recombinant factor VIII (rFVIII) products, including efmoroctocog alfa (fragment crystallizable fusion protein) and rurioctocog alfa pegol (antihemophilic factor [recombinant], PEGylated).
Objective: To evaluate dosing patterns and weekly consumption of extended half-life rFVIII products in the United States.
Methods: We performed a retrospective analysis using the US Specialty Pharmacy Database (2015-2018). Included patients had a diagnosis of hemophilia A, ≥2 consecutive monthly claims for efmoroctocog alfa or rurioctocog alfa pegol for prophylaxis, and weight data. Outcome measures included weekly dosing frequency and dispensed weekly dose.
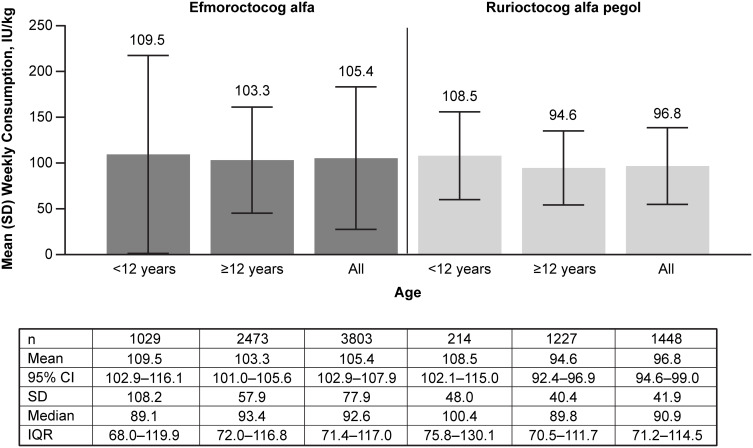
Results: The analysis included 774 patients (efmoroctocog alfa, 506; rurioctocog alfa pegol, 268). Mean (SD) age was 24.2 (15.8) and 26.3 (14.9) years for patients receiving efmoroctocog alfa and rurioctocog alfa pegol, respectively; mean (SD) weight was 68.4 (36.8) and 79.8 (37.7) kg, respectively. The most frequent efmoroctocog alfa regimen was twice weekly (45.7%), followed by every 4 days (20.6%), every 3 days (9.1%), and 3 times per week (7.5%). The most frequent rurioctocog alfa pegol regimen was twice weekly (72.4%), followed by 3 times per week (8.7%), every 4 days (7.6%), and every 3 days (5.5%). The proportion of efmoroctocog alfa twice-weekly dispensing records increased from 31.5% to 50.9%, and every 4 days dispensing records decreased from 31.3% to 14.5% (2015-2018). The proportion of rurioctocog alfa pegol dispensing records remained broadly stable (2016-2018). Overall, mean (SD; median) weekly prophylactic dose was 105.4 (77.9; 92.6) IU/kg with efmoroctocog alfa, and 96.8 (41.9; 90.9) IU/kg with rurioctocog alfa pegol.
Conclusion: In this database study, the most frequently observed dosing frequency was twice weekly for patients receiving efmoroctocog alfa or rurioctocog alfa pegol. The observed mean weekly consumption was slightly higher, and variation was greater, in patients receiving efmoroctocog alfa versus rurioctocog alfa pegol.
Keywords: PEGylated; antihemophilic factor (recombinant); dosing patterns; efmoroctocog alfa; fragment crystallizable fusion protein; hemophilia A; rurioctocog alfa pegol.
© 2022 Wu et al.
Conflict of interest statement
Y. Wu and S.X. Sun are employees of Takeda Development Center Americas, Inc., Cambridge, MA, USA, and Takeda stock owners. T. Fan is an employee of Takeda Pharmaceuticals USA, Inc., Lexington, MA, USA, and Takeda stock owner. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
A Retrospective Observational Study of Rurioctocog Alfa Pegol in Clinical Practice in the United States.J Manag Care Spec Pharm. 2020 Apr;26(4):492-503. doi: 10.18553/jmcp.2020.26.4.492. J Manag Care Spec Pharm. 2020. PMID: 32223610 Free PMC article.
-
Real-world study of rurioctocog alfa pegol and emicizumab in US clinical practice among patients with hemophilia A.Expert Rev Hematol. 2022 Oct;15(10):943-950. doi: 10.1080/17474086.2022.2112171. Epub 2022 Aug 24. Expert Rev Hematol. 2022. PMID: 36000620
-
Clinical efficacy of simoctocog alfa versus extended half-life recombinant FVIII concentrates in hemophilia A patients undergoing personalized prophylaxis using a matching-adjusted indirect comparison method.Eur J Haematol. 2023 Nov;111(5):757-767. doi: 10.1111/ejh.14073. Epub 2023 Aug 16. Eur J Haematol. 2023. PMID: 37587687
-
Damoctocog Alfa Pegol, a PEGylated B-domain Deleted Recombinant Extended Half-life Factor VIII for the Treatment of Hemophilia A: A Product Review.Drugs R D. 2024 Sep;24(3):359-381. doi: 10.1007/s40268-024-00481-7. Epub 2024 Aug 20. Drugs R D. 2024. PMID: 39162954 Free PMC article. Review.
-
Efmoroctocog Alfa: A Review in Haemophilia A.Drugs. 2021 Nov;81(17):2035-2046. doi: 10.1007/s40265-021-01615-w. Epub 2021 Nov 7. Drugs. 2021. PMID: 34743314 Free PMC article. Review.
Cited by
-
Liposomal factor VIII as an efficient pharmaceutical system for the treatment of hemophilia.Iran J Basic Med Sci. 2024;27(6):747-754. doi: 10.22038/IJBMS.2024.74673.16214. Iran J Basic Med Sci. 2024. PMID: 38645492 Free PMC article.
References
-
- Iorio A, Stonebraker JS, Chambost H, et al.; Data Demographics Committee of the World Federation of Hemophilia. Establishing the prevalence and prevalence at birth of hemophilia in males: a meta-analytic approach using national registries. Ann Intern Med. 2019;171(8):540–546. doi:10.7326/M19-1208 - DOI - PubMed
LinkOut - more resources
Full Text Sources
