

Myosteatosis as a Shared Biomarker for Sarcopenia and Cachexia Using MRI and Ultrasound
- PMID: 36189019
- PMCID: PMC9397668
- DOI: 10.3389/fresc.2022.896114
Myosteatosis as a Shared Biomarker for Sarcopenia and Cachexia Using MRI and Ultrasound
Erratum in
-
Corrigendum: Myosteatosis as a Shared Biomarker for Sarcopenia and Cachexia Using MRI and Ultrasound.Front Rehabil Sci. 2022 Jul 15;3:982949. doi: 10.3389/fresc.2022.982949. eCollection 2022. Front Rehabil Sci. 2022. PMID: 36191164 Free PMC article.
Abstract
Purpose: Establish bedside biomarkers of myosteatosis for sarcopenia and cachexia. We compared ultrasound biomarkers against MRI-based percent fat, histology, and CT-based muscle density among healthy adults and adults undergoing treatment for lung cancer.
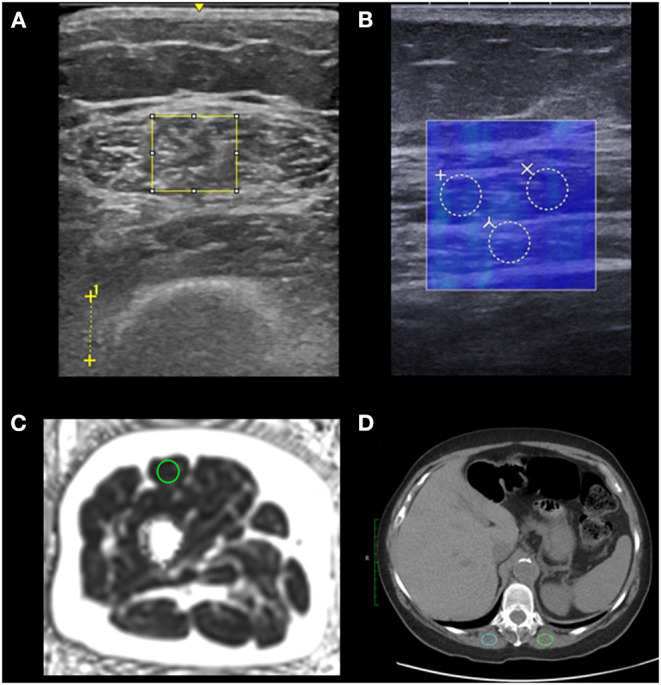
Methods: We compared ultrasound and MRI myosteatosis measures among young healthy, older healthy, and older adults with non-small cell lung cancer undergoing systemic treatment, all without significant medical concerns, in a cross-sectional pilot study. We assessed each participant's rectus femoris ultrasound-based echo intensity (EI), shear wave elastography-based shear wave speed, and MRI-based proton density fat-fraction (PDFF). We also assessed BMI, rectus femoris thickness and cross-sectional area. Rectus femoris biopsies were taken for all older adults (n = 20) and we analyzed chest CT scans for older adults undergoing treatment (n = 10). We determined associations between muscle assessments and BMI, and compared these assessments between groups.
Results: A total of 10 young healthy adults, 10 older healthy adults, and 10 older adults undergoing treatment were recruited. PDFF was lower in young adults than in older healthy adults and older adults undergoing treatment (0.3 vs. 2.8 vs. 2.9%, respectively, p = 0.01). Young adults had significantly lower EI than older healthy adults, but not older adults undergoing treatment (48.6 vs. 81.8 vs. 75.4, p = 0.02). When comparing associations between measures, PDFF was strongly associated with EI (ρ = 0.75, p < 0.01) and moderately negatively associated with shear wave speed (ρ = -0.49, p < 0.01) but not BMI, whole leg cross-sectional area, or rectus femoris cross-sectional area. Among participants with CT scans, paraspinal muscle density was significantly associated with PDFF (ρ = -0.70, p = 0.023). Histological markers of inflammation or degradation did not differ between older adult groups.
Conclusion: PDFF was sensitive to myosteatosis between young adults and both older adult groups. EI was less sensitive to myosteatosis between groups, yet EI was strongly associated with PDFF unlike BMI, which is typically used in cachexia diagnosis. Our results suggest that ultrasound measures may serve to determine myosteatosis at the bedside and are more useful diagnostically than traditional weight assessments like BMI. These results show promise of using EI, shear wave speed, and PDFF proxies of myosteatosis as diagnostic and therapeutic biomarkers of sarcopenia and cachexia.
Keywords: MRI; cancer; echo intensity; elasticity; muscle health; muscle quality; proton density fat fraction; ultrasound.
Copyright © 2022 Lortie, Rush, Osterbauer, Colgan, Tamada, Garlapati, Campbell, Traynor, Leal, Patel, Helgager, Lee, Reeder and Kuchnia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources