

Mechanisms of tumor resistance to immune checkpoint blockade and combination strategies to overcome resistance
- PMID: 36189283
- PMCID: PMC9520263
- DOI: 10.3389/fimmu.2022.915094
Mechanisms of tumor resistance to immune checkpoint blockade and combination strategies to overcome resistance
Abstract
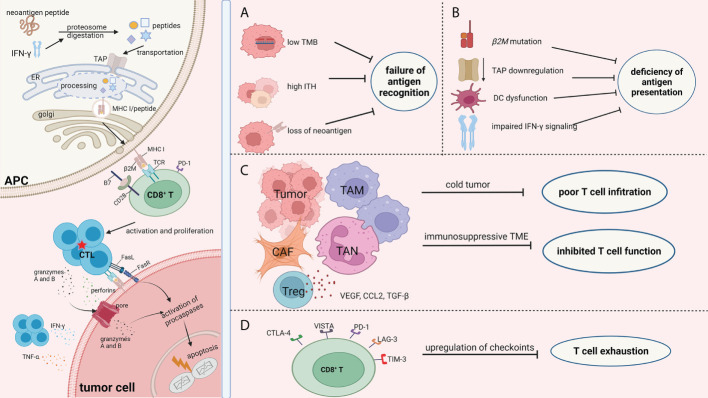
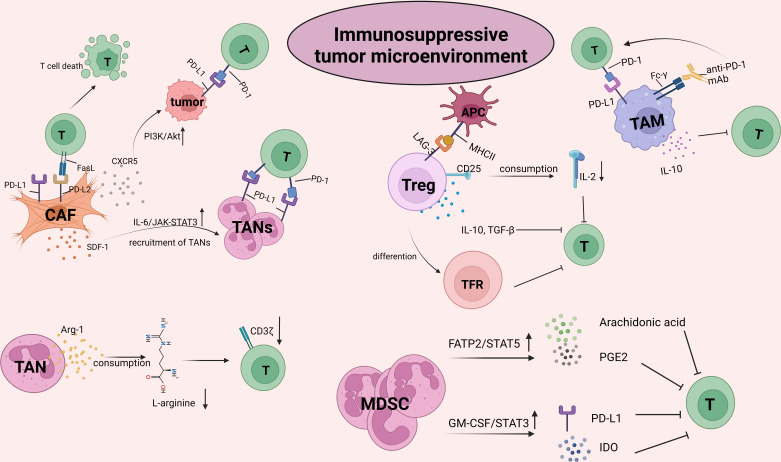
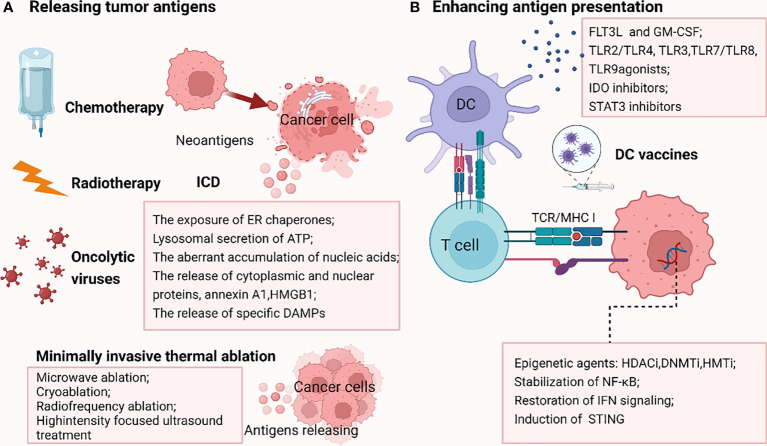
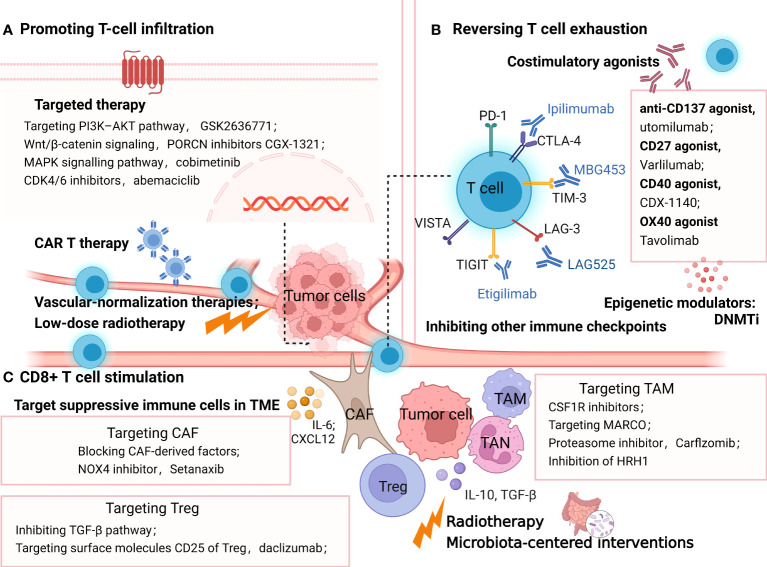
Immune checkpoint blockade (ICB) has rapidly transformed the treatment paradigm for various cancer types. Multiple single or combinations of ICB treatments have been approved by the US Food and Drug Administration, providing more options for patients with advanced cancer. However, most patients could not benefit from these immunotherapies due to primary and acquired drug resistance. Thus, a better understanding of the mechanisms of ICB resistance is urgently needed to improve clinical outcomes. Here, we focused on the changes in the biological functions of CD8+ T cells to elucidate the underlying resistance mechanisms of ICB therapies and summarized the advanced coping strategies to increase ICB efficacy. Combinational ICB approaches and individualized immunotherapies require further in-depth investigation to facilitate longer-lasting efficacy and a more excellent safety of ICB in a broader range of patients.
Keywords: T cell response; combination therapy; immune checkpoint blockade; immunotherapy; resistance mechanisms.
Copyright © 2022 Zhou, Ni, Liang, Lin, An, He and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials