

Right ventricular strain measurements in critically ill patients: an observational SICS sub-study
- PMID: 36190597
- PMCID: PMC9530097
- DOI: 10.1186/s13613-022-01064-y
Right ventricular strain measurements in critically ill patients: an observational SICS sub-study
Abstract
Background: Right ventricular (RV) dysfunction is common in critically ill patients and is associated with poor outcomes. RV function is usually evaluated by Tricuspid Annular Plane Systolic Excursion (TAPSE) which can be obtained using critical care echocardiography (CCE). Myocardial deformation imaging, measuring strain, is suitable for advanced RV function assessment and has widely been studied in cardiology. However, it is relatively new for the Intensive Care Unit (ICU) and little is known about RV strain in critically ill patients. Therefore, the objectives of this study were to evaluate the feasibility of RV strain in critically ill patients using tissue-Doppler imaging (TDI) and explore the association between RV strain and conventional CCE measurements representing RV function.
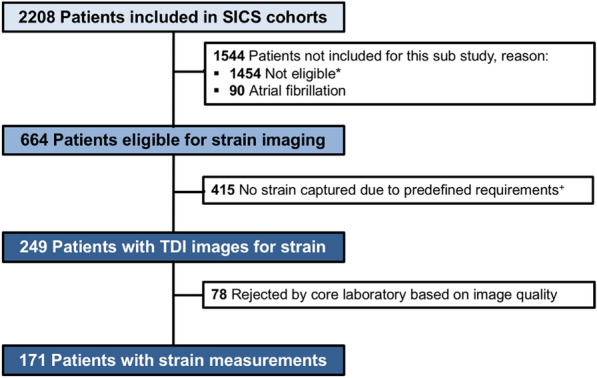
Methods: This is a single-center sub-study of two prospective observational cohorts (Simple Intensive Care Studies (SICS)-I and SICS-II). All acutely admitted adults with an expected ICU stay over 24 h were included. CCE was performed within 24 h of ICU admission. In patients in which CCE was performed, TAPSE, peak systolic velocity at the tricuspid annulus (RV s') and TDI images were obtained. RV free wall longitudinal strain (RVFWSL) and RV global four-chamber longitudinal strain (RV4CSL) were measured during offline analysis.
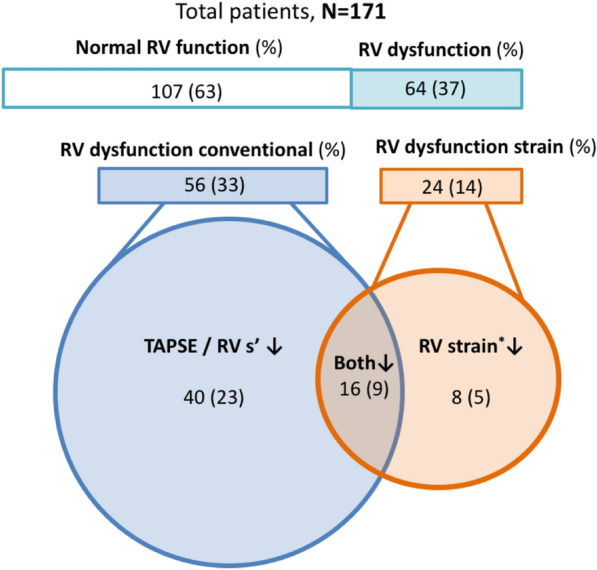
Results: A total of 171 patients were included. Feasibility of RVFWSL and RV4CSL was, respectively, 62% and 56% in our population; however, when measurements were performed, intra- and inter-rater reliability based on the intraclass correlation coefficient were good to excellent. RV dysfunction based on TAPSE or RV s' was found in 56 patients (33%) and 24 patients (14%) had RV dysfunction based on RVFWSL or RV4CSL. In 14 patients (8%), RVFWSL, RV4CSL, or both were reduced, despite conventional RV function measurements being preserved. These patients had significantly higher severity of illness scores. Sensitivity analysis with fractional area change showed similar results.
Conclusions: TDI RV strain imaging in critically ill patients is challenging; however, good-to-excellent reproducibility was shown when measurements were adequately obtained. Future studies are needed to elucidate the diagnostic and prognostic value of RV strain in critically ill patients, especially to outweigh the difficulty and effort of imaging against the clinical value.
Keywords: Critical care; Echocardiography; Prospective study; Right ventricular function; Strain imaging.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713. doi: 10.1016/j.echo.2010.05.010. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
