

Change in healthcare utilisation after surgical treatment: observational study of routinely collected patient data from primary and secondary care
- PMID: 36192218
- PMCID: PMC9748995
- DOI: 10.1016/j.bja.2022.07.012
Change in healthcare utilisation after surgical treatment: observational study of routinely collected patient data from primary and secondary care
Abstract
Background: Most patients fully recover after surgery. However, high-risk patients may experience an increased burden of medical disease.
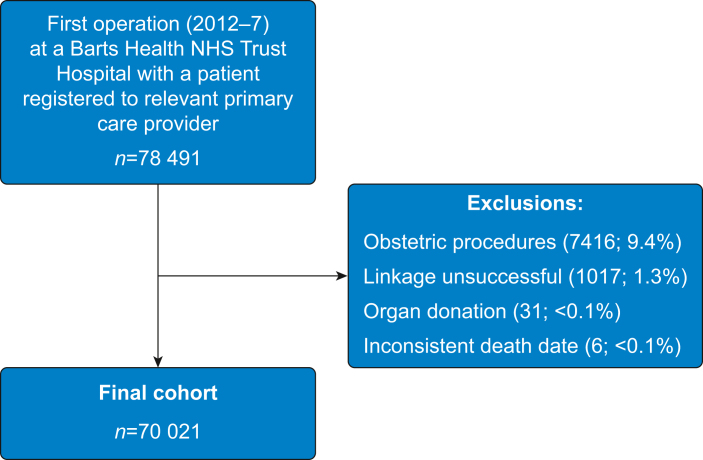
Methods: We performed a prospectively planned analysis of linked routine primary and secondary care data describing adult patients undergoing non-obstetric surgery at four hospitals in East London between January 2012 and January 2017. We categorised patients by 90-day mortality risk using logistic regression modelling. We calculated healthcare contact days per patient year during the 2 yr before and after surgery, and express change using rate ratios (RaR) with 95% confidence intervals.
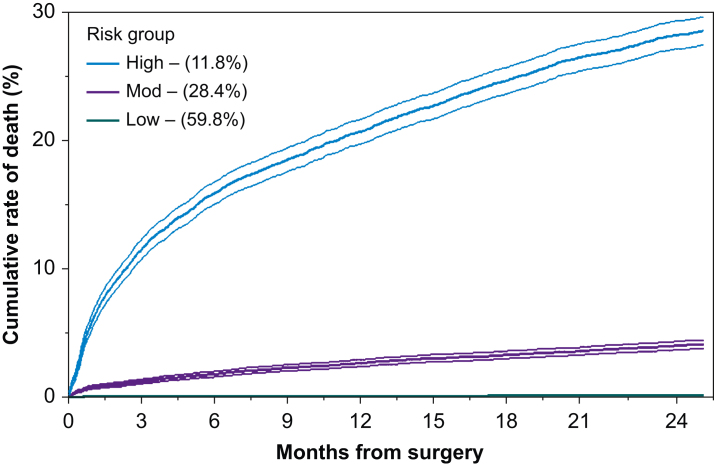
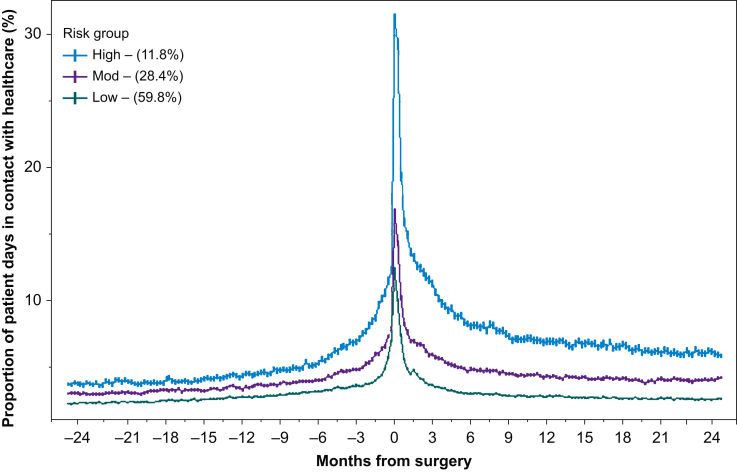
Results: We included 70 021 patients, aged (mean [standard deviation, sd]) 49.8 (19) yr, with 1238 deaths within 2 yr after surgery (1.8%). Most procedures were elective (51 693, 74.0%), and 20 441 patients (29.1%) were in the most deprived national quintile for social deprivation. Elective patients had 12.7 healthcare contact days per patient year before surgery, increasing to 15.5 days in the 2 yr after surgery (RaR, 1.22 [1.21-1.22]), and those at high-risk of 90-day mortality (11% of population accounting for 80% of all deaths) had the largest increase (37.0 days per patient year before vs 60.8 days after surgery; RaR, 1.64 [1.63-1.65]). Emergency patients had greater increases in healthcare burden (13.8 days per patient year before vs 24.8 days after surgery; RaR, 1.8 [1.8-1.8]), particularly in high-risk patients (28% of patients accounting for 80% of all deaths by day 90), with 21.6 days per patient year before vs 49.2 days after surgery; RaR, 2.28 [2.26-2.29].
Discussion: High-risk patients who survive the immediate perioperative period experience large and persistent increases in healthcare utilisation in the years after surgery. The full implications of this require further study.
Keywords: anaesthesia; complications; healthcare cost; peri-operative medicine; primary care; surgery.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Changes in healthcare utilisation after surgical treatment: mitigating risk through multidisciplinary and collaborative care.Br J Anaesth. 2022 Dec;129(6):840-842. doi: 10.1016/j.bja.2022.09.015. Epub 2022 Nov 1. Br J Anaesth. 2022. PMID: 36333162
Similar articles
-
Long-term healthcare use after postoperative complications: an analysis of linked primary and secondary care routine data.BJA Open. 2023 Jun 15;7:100142. doi: 10.1016/j.bjao.2023.100142. eCollection 2023 Sep. BJA Open. 2023. PMID: 37638082 Free PMC article.
-
Patterns of healthcare utilisation in children and young people: a retrospective cohort study using routinely collected healthcare data in Northwest London.BMJ Open. 2021 Dec 17;11(12):e050847. doi: 10.1136/bmjopen-2021-050847. BMJ Open. 2021. PMID: 34921075 Free PMC article.
-
Outcomes after surgery for children in Africa (ASOS-Paeds): a 14-day prospective observational cohort study.Lancet. 2024 Apr 13;403(10435):1482-1492. doi: 10.1016/S0140-6736(24)00103-X. Epub 2024 Mar 22. Lancet. 2024. PMID: 38527482
-
Perioperative alcohol cessation intervention for postoperative complications.Cochrane Database Syst Rev. 2018 Nov 8;11(11):CD008343. doi: 10.1002/14651858.CD008343.pub3. Cochrane Database Syst Rev. 2018. PMID: 30408162 Free PMC article.
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
Cited by
-
Long-term healthcare use after postoperative complications: an analysis of linked primary and secondary care routine data.BJA Open. 2023 Jun 15;7:100142. doi: 10.1016/j.bjao.2023.100142. eCollection 2023 Sep. BJA Open. 2023. PMID: 37638082 Free PMC article.
-
Rives-Stoppa Repair Versus Bilateral Inguinal Hernioplasty: A Comprehensive Review of Surgical Techniques and Patient Outcomes.Cureus. 2024 Jul 26;16(7):e65439. doi: 10.7759/cureus.65439. eCollection 2024 Jul. Cureus. 2024. PMID: 39184704 Free PMC article. Review.
References
-
- Abbott T.E.F., Fowler A.J., Dobbs T.D., Harrison E.M., Gillies M.A., Pearse R.M. Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics. Br J Anaesth. 2017;119:249–257. - PubMed
-
- Fowler A.J., Abbott T.E.F., Prowle J., Pearse R.M. Age of patients undergoing surgery. Br J Surg Engl. 2019;106:1012–1018. - PubMed
-
- Wan Y.I., McGuckin D., Fowler A.J., Prowle J.R., Pearse R.M., Moonesinghe S.R. Socioeconomic deprivation and long-term outcomes after elective surgery: analysis of prospective data from two observational studies. Br J Anaesth. 2021;126:642–651. - PubMed
-
- Toner A., Hamilton M. The long-term effects of postoperative complications. Curr Opin Crit Care. 2013;19:364–368. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
