

Sevoflurane dose and postoperative delirium: a prospective cohort analysis
- PMID: 36192219
- PMCID: PMC9997074
- DOI: 10.1016/j.bja.2022.08.022
Sevoflurane dose and postoperative delirium: a prospective cohort analysis
Abstract
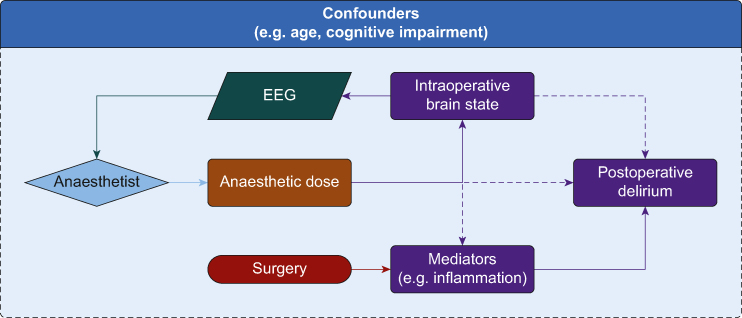
Background: Recent trials are conflicting as to whether titration of anaesthetic dose using electroencephalography monitoring reduces postoperative delirium. Titration to anaesthetic dose itself might yield clearer conclusions. We analysed our observational cohort to clarify both dose ranges for trials of anaesthetic dose and biological plausibility of anaesthetic dose influencing delirium.
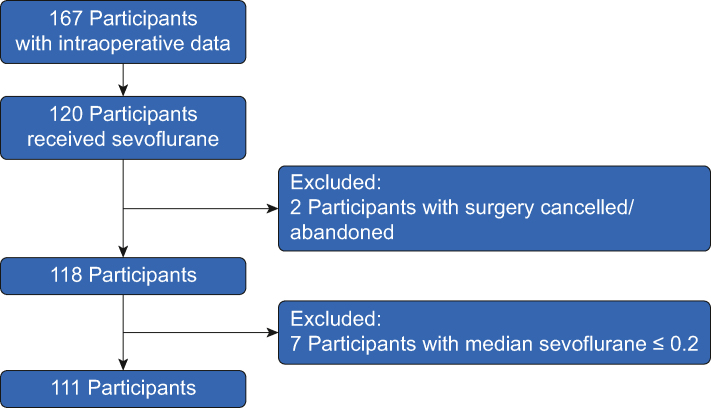
Methods: We analysed the use of sevoflurane in an ongoing prospective cohort of non-intracranial surgery. Of 167 participants, 118 received sevoflurane and were aged >65 yr. We tested associations between age-adjusted median sevoflurane (AMS) minimum alveolar concentration fraction or area under the sevoflurane time×dose curve (AUC-S) and delirium severity (Delirium Rating Scale-98). Delirium incidence was measured with 3-minute Diagnostic Confusion Assessment Method (3D-CAM) or CAM-ICU. Associations with previously identified delirium biomarkers (interleukin-8, neurofilament light, total tau, or S100B) were tested.
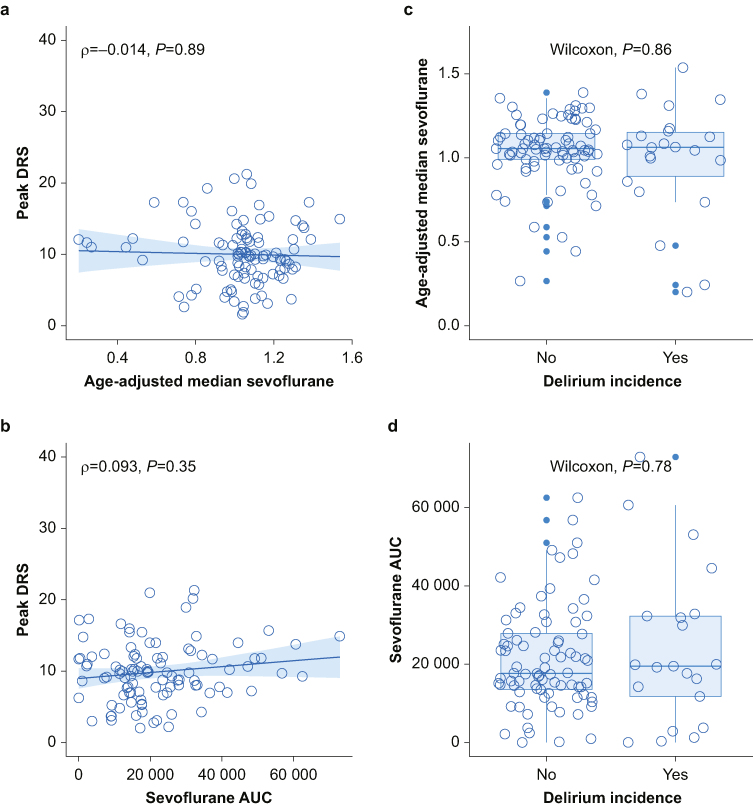
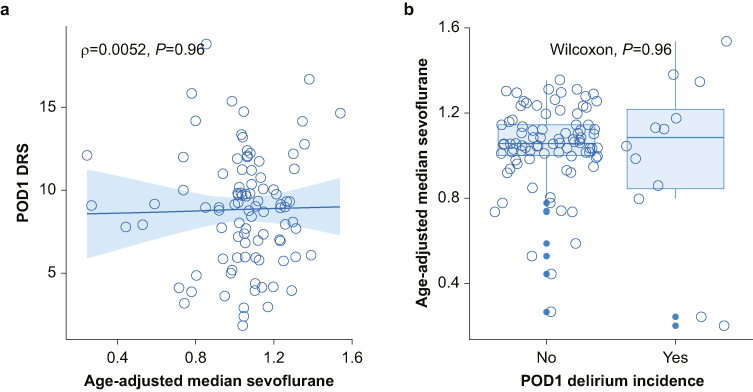
Results: Delirium severity did not correlate with AMS (Spearman's ρ=-0.014, P=0.89) or AUC-S (ρ=0.093, P=0.35), nor did delirium incidence (AMS Wilcoxon P=0.86, AUC-S P=0.78). Further sensitivity analyses including propofol dose also demonstrated no relationship. Linear regression confirmed no association for AMS in unadjusted (log (IRR)=-0.06 P=0.645) or adjusted models (log (IRR)=-0.0454, P=0.735). No association was observed for AUC-S in unadjusted (log (IRR)=0.00, P=0.054) or adjusted models (log (IRR)=0.00, P=0.832). No association of anaesthetic dose with delirium biomarkers was identified (P>0.05).
Conclusion: Sevoflurane dose was not associated with delirium severity or incidence. Other biological mechanisms of delirium, such as inflammation and neuronal injury, appear more plausible than dose of sevoflurane.
Clinical trial registration: NCT03124303, NCT01980511.
Keywords: anaesthesia; biomarker; cognitive dysfunction; delirium; dose dependency; postoperative; sevoflurane; surgery.
Copyright © 2022 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Sevoflurane dose and postoperative delirium. Comment on Br J Anaesth 2023; 130: e289-97.Br J Anaesth. 2023 Jun;130(6):e481-e482. doi: 10.1016/j.bja.2023.02.010. Epub 2023 Mar 15. Br J Anaesth. 2023. PMID: 36931961 No abstract available.
References
-
- Gaskell A., Sleigh J. The quagmire of postoperative delirium: does dose matter? Br J Anaesth. 2021;127:664–666. - PubMed
-
- Whitlock E.L., Gross E.R., King C.R., Avidan M.S. Anaesthetic depth and delirium: a challenging balancing act. Br J Anaesth. 2021;127:667–671. - PubMed
-
- Chan M.T., Cheng B.C., Lee T.M., Gin T., Group C.T. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol. 2013;25:33–42. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
