

Lessening the Impact of Financial Toxicity (LIFT): a protocol for a multi-site, single-arm trial examining the effect of financial navigation on financial toxicity in adult patients with cancer in rural and non-rural settings
- PMID: 36192802
- PMCID: PMC9527389
- DOI: 10.1186/s13063-022-06745-4
Lessening the Impact of Financial Toxicity (LIFT): a protocol for a multi-site, single-arm trial examining the effect of financial navigation on financial toxicity in adult patients with cancer in rural and non-rural settings
Abstract
Background: Almost half of the patients with cancer report cancer-related financial hardship, termed "financial toxicity" (FT), which affects health-related quality of life, care retention, and, in extreme cases, mortality. This increasingly prevalent hardship warrants urgent intervention. Financial navigation (FN) targets FT by systematically identifying patients at high risk, assessing eligibility for existing resources, clarifying treatment cost expectations, and working with patients and caregivers to develop a plan to cope with cancer costs. This trial seeks to (1) identify FN implementation determinants and implementation outcomes, and (2) evaluate the effectiveness of FN in improving patient outcomes.
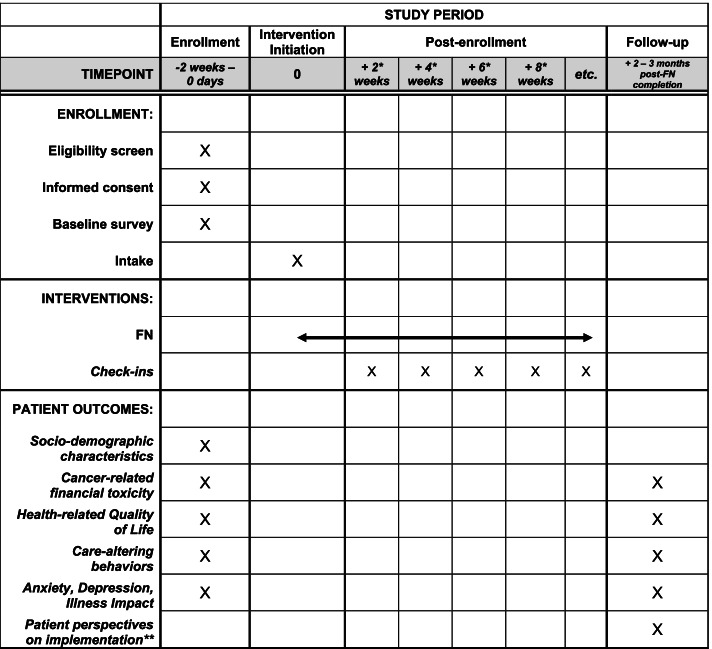
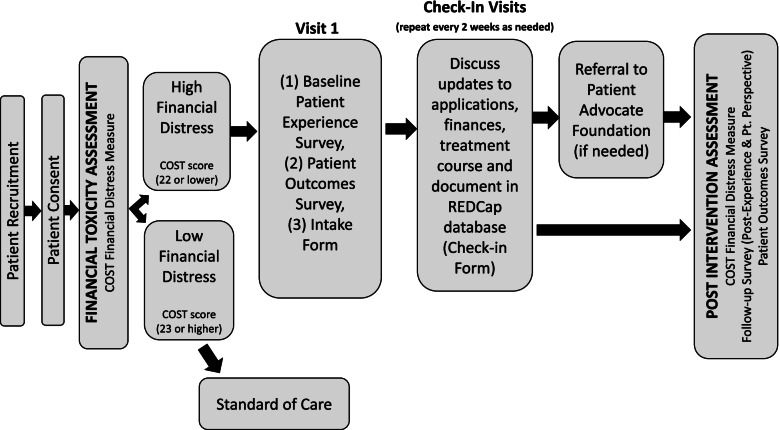
Methods: The Lessening the Impact of Financial Toxicity (LIFT) study is a multi-site Phase 2 clinical trial. We use a pre-/post- single-arm intervention to examine the effect of FN on FT in adults with cancer. The LIFT trial is being conducted at nine oncology care settings across North Carolina in the United States. Sites vary in geography (five rural, four non-rural), size (21-974 inpatient beds), and ownership structure (governmental, non-profit). The study will enroll 780 patients total over approximately 2 years. Eligible patients must be 18 years or older, have a confirmed cancer diagnosis (any type) within the past 5 years or be living with advanced disease, and screen positive for cancer-related financial distress. LIFT will be delivered by full- or part-time financial navigators and consists of 3 components: (1) systematic FT screening identification and comprehensive intake assessment; (2) connecting patients experiencing FT to financial support resources via trained oncology financial navigators; and (3) ongoing check-ins and electronic tracking of patients' progress and outcomes by financial navigators. We will measure intervention effectiveness by evaluating change in FT (via the validated Comprehensive Score of Financial Toxicity, or COST instrument) (primary outcome), as well as health-related quality of life (PROMIS Global Health Questionnaire), and patient-reported delayed or forgone care due to cost. We also assess patient- and stakeholder-reported implementation and service outcomes post-intervention, including uptake, fidelity, acceptability, cost, patient-centeredness, and timeliness.
Discussion: This study adds to the growing evidence on FN by evaluating its implementation and effectiveness across diverse oncology care settings.
Trial registration: ClinicalTrials.gov NCT04931251. Registered on June 18, 2021.
Keywords: Cancer; Financial navigation; Financial toxicity; Multi-site behavioral intervention.
© 2022. The Author(s).
Conflict of interest statement
SBW, DLR, KRH, CSR, MM, MG, and NP have received funding paid to their institution from the Pfizer Foundation. LPS and SBW have received funding paid to their institution from AstraZeneca.
Figures
References
-
- Zafar SY, Abernethy AP. Financial toxicity, Part II: how can we help with the burden of treatment-related costs? Oncology (Williston Park) 2013;27(4):253–254. - PubMed
-
- Kazzi B, Chino F, Kazzi B, Jain B, Tian S, Paguio JA, et al. Shared burden: the association between cancer diagnosis, financial toxicity, and healthcare cost-related coping mechanisms by family members of non-elderly patients in the USA. Support Care Cancer. 2022. Epub ahead of print. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
