Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach
- PMID: 36193717
- PMCID: PMC9633223
- DOI: 10.3803/EnM.2022.1553
Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach
Abstract
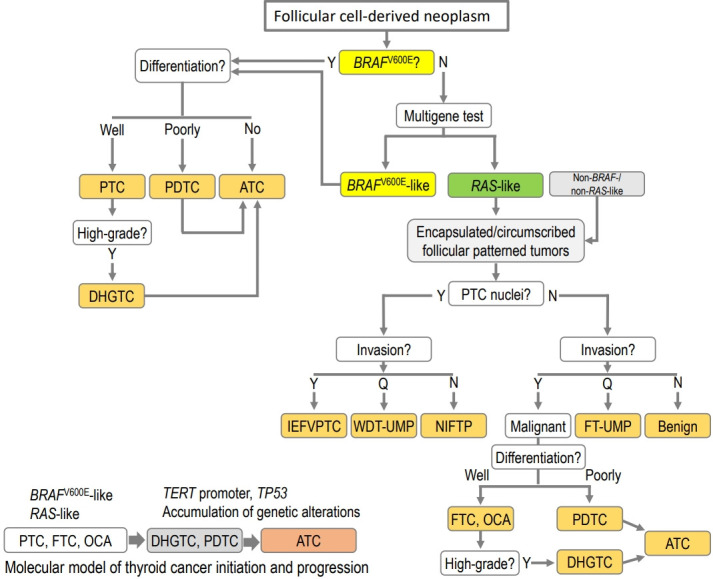
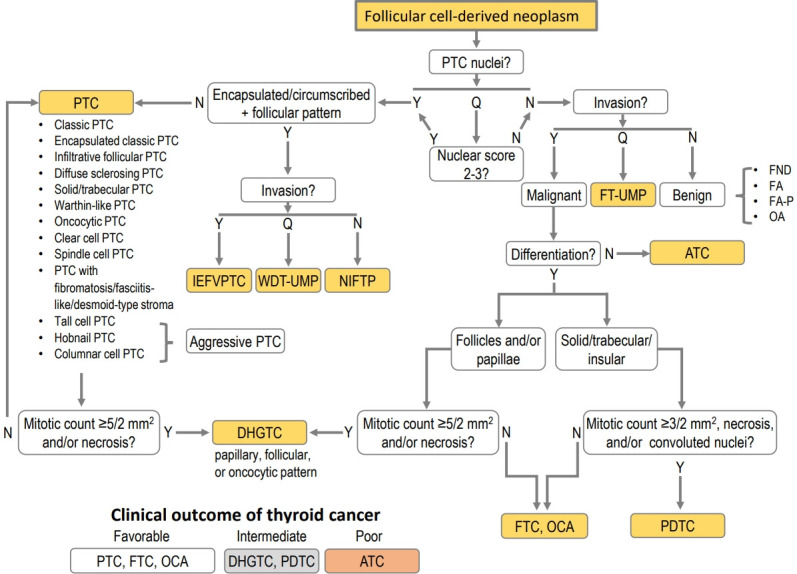
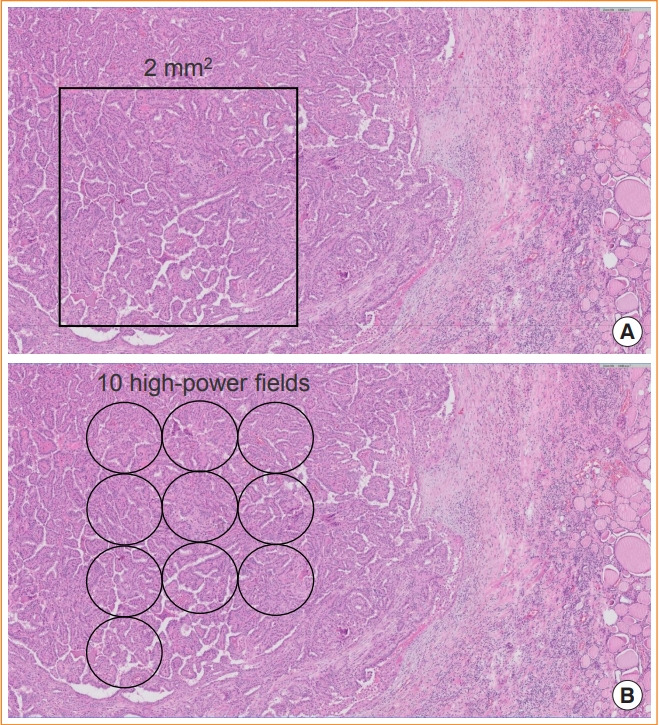
The fifth edition of the World Health Organization (WHO) histologic classification of thyroid neoplasms released in 2022 includes newly recognized tumor types, subtypes, and a grading system. Follicular cell-derived neoplasms are categorized into three families (classes): benign tumors, low-risk neoplasms, and malignant neoplasms. The terms "follicular nodular disease" and "differentiated high-grade thyroid carcinoma" are introduced to account for multifocal hyperplastic/neoplastic lesions and differentiated thyroid carcinomas with high-grade features, respectively. The term "Hürthle cells" is replaced with "oncocytic cells." Invasive encapsulated follicular and cribriform morular variants of papillary thyroid carcinoma (PTC) are now redefined as distinct tumor types, given their different genetic alterations and clinicopathologic characteristics from other PTC subtypes. The term "variant" to describe a subclass of tumor has been replaced with the term "subtype." Instead, the term "variant" is reserved to describe genetic alterations. A histologic grading system based on the mitotic count, necrosis, and/or the Ki67 index is used to identify high-grade follicular-cell derived carcinomas and medullary thyroid carcinomas. The 2022 WHO classification introduces the following new categories: "salivary gland-type carcinomas of the thyroid" and "thyroid tumors of uncertain histogenesis." This review summarizes the major changes in the 2022 WHO classification and their clinical relevance.
Keywords: Classification; Standards; Thyroid neoplasms; Thyroid nodule; World Health Organization.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Overview of the 2022 WHO Classification of Thyroid Neoplasms.Endocr Pathol. 2022 Mar;33(1):27-63. doi: 10.1007/s12022-022-09707-3. Epub 2022 Mar 14. Endocr Pathol. 2022. PMID: 35288841 Review.
-
The 2022 WHO classification of thyroid tumors: novel concepts in nomenclature and grading.Endocr Relat Cancer. 2022 Dec 22;30(2):e220293. doi: 10.1530/ERC-22-0293. Print 2023 Feb 1. Endocr Relat Cancer. 2022. PMID: 36445235 Review.
-
Changes in the diagnosis of thyroid tumours in the 5th edition of the WHO classification of endocrine neoplasms.Cesk Patol. 2024;60(1):59-63. Cesk Patol. 2024. PMID: 38697828 Review. English.
-
WHO 2022 updates on follicular cell and c-cell derived thyroid neoplasm.J Med Life. 2024 Jan;17(1):15-23. doi: 10.25122/jml-2023-0270. J Med Life. 2024. PMID: 38737660 Free PMC article.
-
Follicular histotypes of oncocytic thyroid carcinomas do not carry mutations of the BRAF hot-spot.World J Surg. 2008 May;32(5):722-8. doi: 10.1007/s00268-007-9431-6. World J Surg. 2008. PMID: 18235983
Cited by
-
Prognosis of Poorly Differentiated Thyroid Carcinoma: A Systematic Review and Meta-Analysis.Endocrinol Metab (Seoul). 2024 Aug;39(4):590-602. doi: 10.3803/EnM.2024.1927. Epub 2024 Jun 27. Endocrinol Metab (Seoul). 2024. PMID: 38925909 Free PMC article.
-
Current and future of immunotherapy for thyroid cancer based on bibliometrics and clinical trials.Discov Oncol. 2024 Feb 25;15(1):50. doi: 10.1007/s12672-024-00904-6. Discov Oncol. 2024. PMID: 38403820 Free PMC article. Review.
-
Agrin is a novel oncogenic protein in thyroid cancer.Oncol Lett. 2023 Sep 25;26(5):483. doi: 10.3892/ol.2023.14070. eCollection 2023 Nov. Oncol Lett. 2023. PMID: 37818129 Free PMC article.
-
Cytology and Histology of Thyroid Nodules: Exploring Novel Insights in the Molecular Era for Enhanced Patient Management.Curr Oncol. 2023 Aug 21;30(8):7753-7772. doi: 10.3390/curroncol30080562. Curr Oncol. 2023. PMID: 37623043 Free PMC article. Review.
-
Ultrasound evolution of parenchymal changes in the thyroid gland with autoimmune thyroiditis in children prior to the development of papillary thyroid carcinoma - a follow-up study.Front Endocrinol (Lausanne). 2023 Apr 12;14:1172823. doi: 10.3389/fendo.2023.1172823. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37124746 Free PMC article.
References
-
- Lloyd RV, Osamura RY, Kloppel G, Rosai J. WHO classification of tumours of endocrine organs. 4th ed. Lyon: International Agency for Research on Cancer (IARC); 2017. pp. 65–91.
-
- Kakudo K, Bychkov A, Bai Y, Li Y, Liu Z, Jung CK. The new 4th edition World Health Organization classification for thyroid tumors, Asian perspectives. Pathol Int. 2018;68:641–64. - PubMed
-
- WHO Classification of Tumours Editorial Board . Lyon: International Agency for Research on Cancer; 2022. Endocrine and neuroendocrine tumours [Internet] [cited 2022 Sep 19]. Available from: https://tumourclassification.iarc.who.int/chapters/36.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical