

Incidence and Outcomes of Advanced Heart Failure in Adults With Congenital Heart Disease
- PMID: 36193744
- PMCID: PMC9760468
- DOI: 10.1161/CIRCHEARTFAILURE.122.009675
Incidence and Outcomes of Advanced Heart Failure in Adults With Congenital Heart Disease
Abstract
Background: There are limited data about the stage D heart failure (advanced HF) in adults with congenital heart disease. Our study objectives were (1) to determine the incidence of new-onset advanced HF in patients and the relationship between advanced HF and all-cause mortality and (2) to determine the relationship between therapies for advanced HF and all-cause mortality.
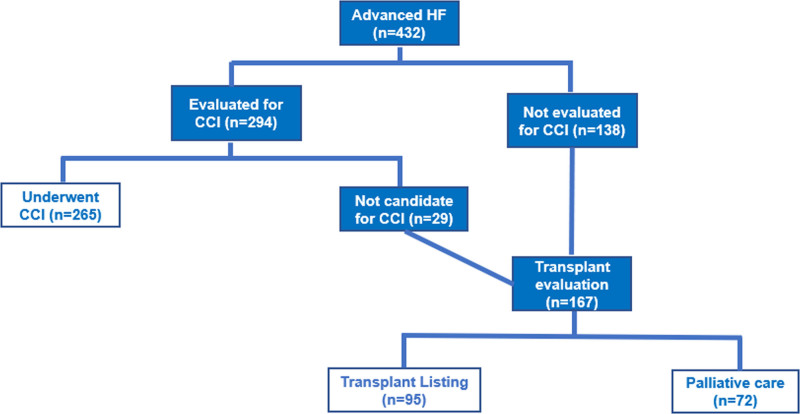
Methods: Retrospective cohort study of adults with congenital heart disease at Mayo Clinic (2003-2019). We defined advanced HF using the European Society of Cardiology diagnostic criteria for advanced HF. Therapies received by the patients with advanced HF were classified into 3 mutually exclusive groups (treatment pathways): (1) conventional cardiac intervention, (2) transplant listing, and (3) palliative care.
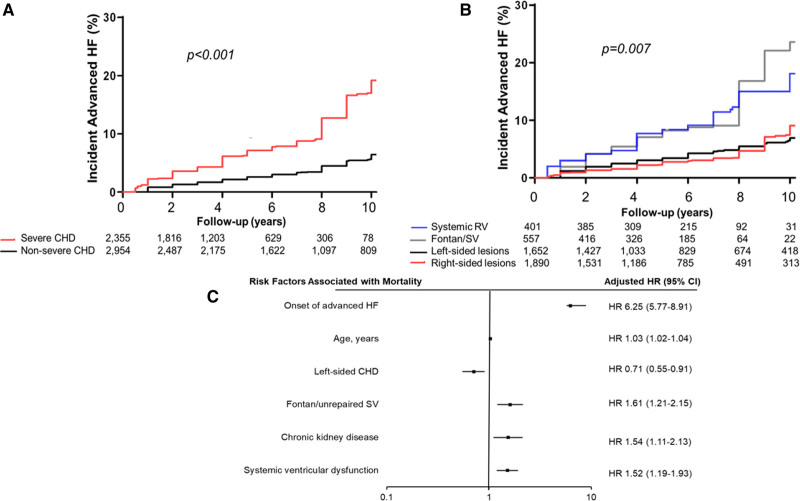
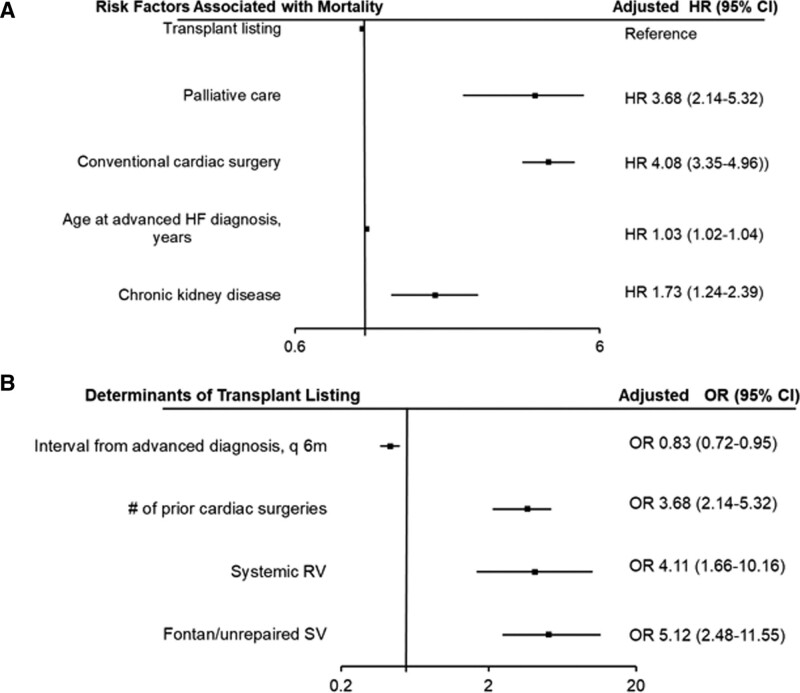
Results: Of 5309 patients without advanced HF at baseline assessment, 432 (8%) developed advanced HF during follow-up (1.1%/y), and the incidence of advanced HF was higher in patients with severe or complex congenital heart disease. Onset of advanced HF was associated with 6-fold increase in the risk of mortality. Conventional cardiac intervention was associated with significantly higher risk of mortality as compared to transplant listing. The longer the interval from the initial onset of advanced HF to transplant evaluation, the lower the odds of being listed for transplant.
Conclusions: Based on these data, we postulate that early identification of patients with advanced HF, and a timely referral for transplant evaluation (instead of conventional cardiac intervention) may offer the best chance of survival for these critically ill patients. Further studies are required to validate this postulation.
Keywords: adults; heart disease; heart failure; incidence; mortality.
Figures
Comment in
-
Calling for Cooperation and Collaboration in Adult Congenital Heart Disease-Related Heart Failure.Circ Heart Fail. 2022 Dec;15(12):e010063. doi: 10.1161/CIRCHEARTFAILURE.122.010063. Epub 2022 Oct 4. Circ Heart Fail. 2022. PMID: 36193747 No abstract available.
References
-
- Diller GP, Kempny A, Alonso-Gonzalez R, Swan L, Uebing A, Li W, Babu-Narayan S, Wort SJ, Dimopoulos K, Gatzoulis MA. Survival prospects and circumstances of death in contemporary adult congenital heart disease patients under follow-up at a large tertiary centre. Circulation. 2015;132:2118–2125. doi: 10.1161/CIRCULATIONAHA.115.017202 - PubMed
-
- Verheugt CL, Uiterwaal CS, van der Velde ET, Meijboom FJ, Pieper PG, van Dijk AP, Vliegen HW, Grobbee DE, Mulder BJ. Mortality in adult congenital heart disease. Eur Heart J. 2010;31:1220–1229. doi: 10.1093/eurheartj/ehq032 - PubMed
-
- Zomer AC, Vaartjes I, van der Velde ET, de Jong HM, Konings TC, Wagenaar LJ, Heesen WF, Eerens F, Baur LH, Grobbee DE, et al. Heart failure admissions in adults with congenital heart disease; risk factors and prognosis. Int J Cardiol. 2013;168:2487–2493. doi: 10.1016/j.ijcard.2013.03.003 - PubMed
-
- Engelings CC, Helm PC, Abdul-Khaliq H, Asfour B, Bauer UM, Baumgartner H, Kececioglu D, Körten MA, Diller GP, Tutarel O. Cause of death in adults with congenital heart disease - an analysis of the German National Register for Congenital Heart Defects. Int J Cardiol. 2016;211:31–36. doi: 10.1016/j.ijcard.2016.02.133 - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, et al. ; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–e239. doi: 10.1016/j.jacc.2013.05.019 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
