

Guideline-Directed Medical Therapy Attainment and Outcomes in Dialysis-Requiring Versus Nondialysis Chronic Kidney Disease in the ISCHEMIA-CKD Trial
- PMID: 36193750
- PMCID: PMC9588677
- DOI: 10.1161/CIRCOUTCOMES.122.008995
Guideline-Directed Medical Therapy Attainment and Outcomes in Dialysis-Requiring Versus Nondialysis Chronic Kidney Disease in the ISCHEMIA-CKD Trial
Abstract
Background: Patients with chronic kidney disease (CKD) on dialysis (CKD G5D) have worse cardiovascular outcomes than patients with advanced nondialysis CKD (CKD G4-5: estimated glomerular filtration rate <30 mL/[min·1.73m2]). Our objective was to evaluate the relationship between achievement of cardiovascular guideline-directed medical therapy (GDMT) goals and clinical outcomes for CKD G5D versus CKD G4-5.
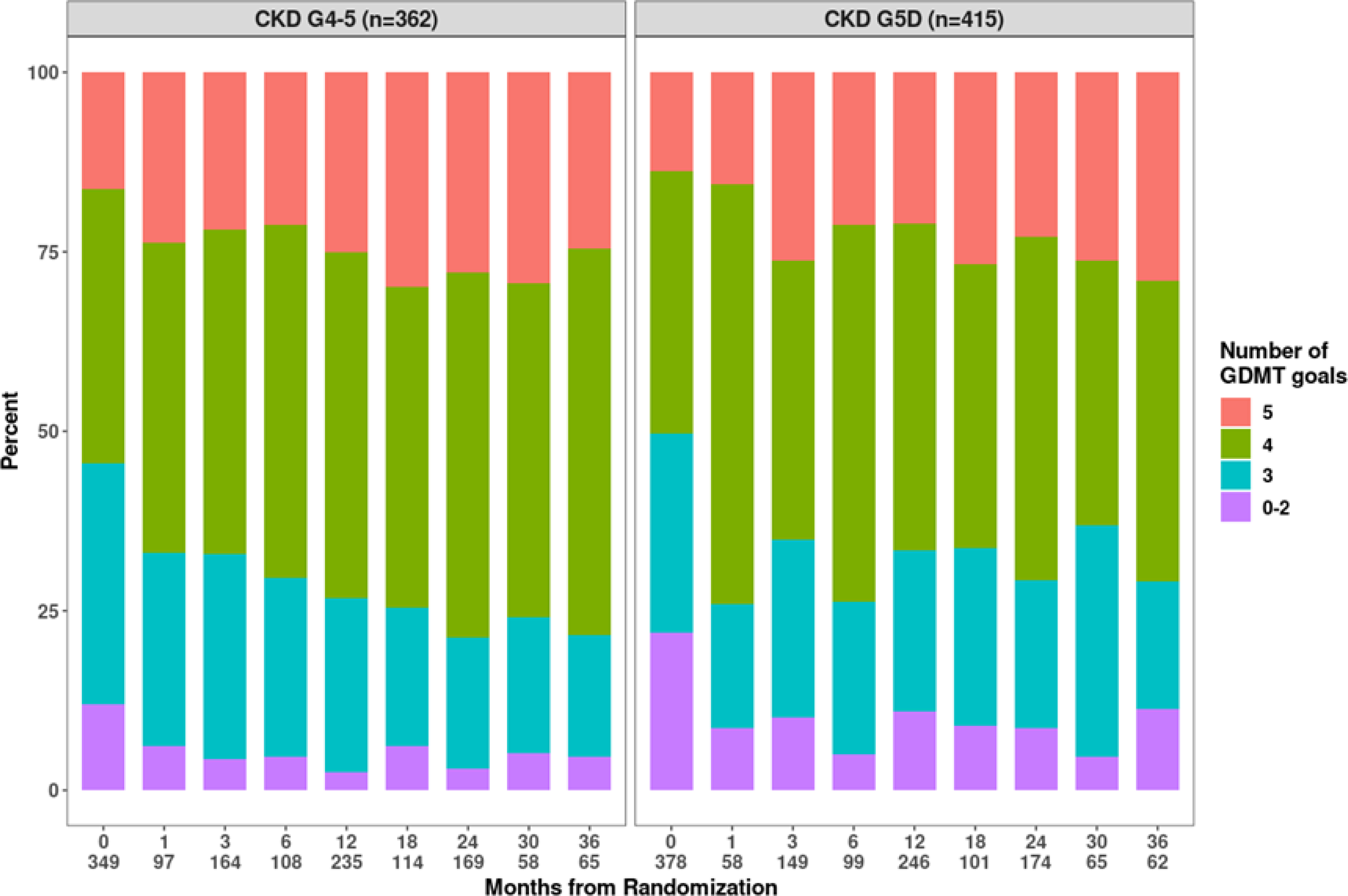
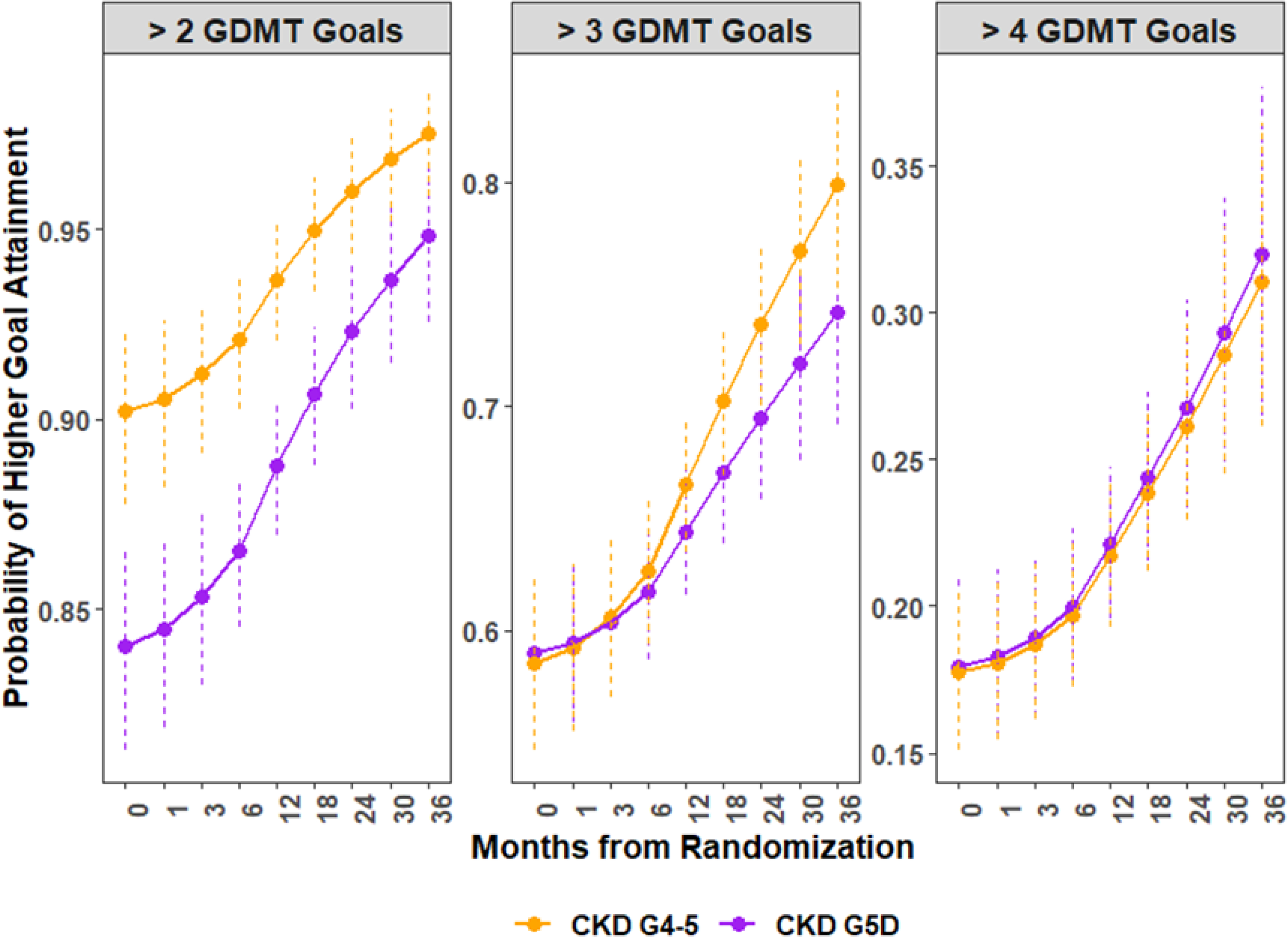
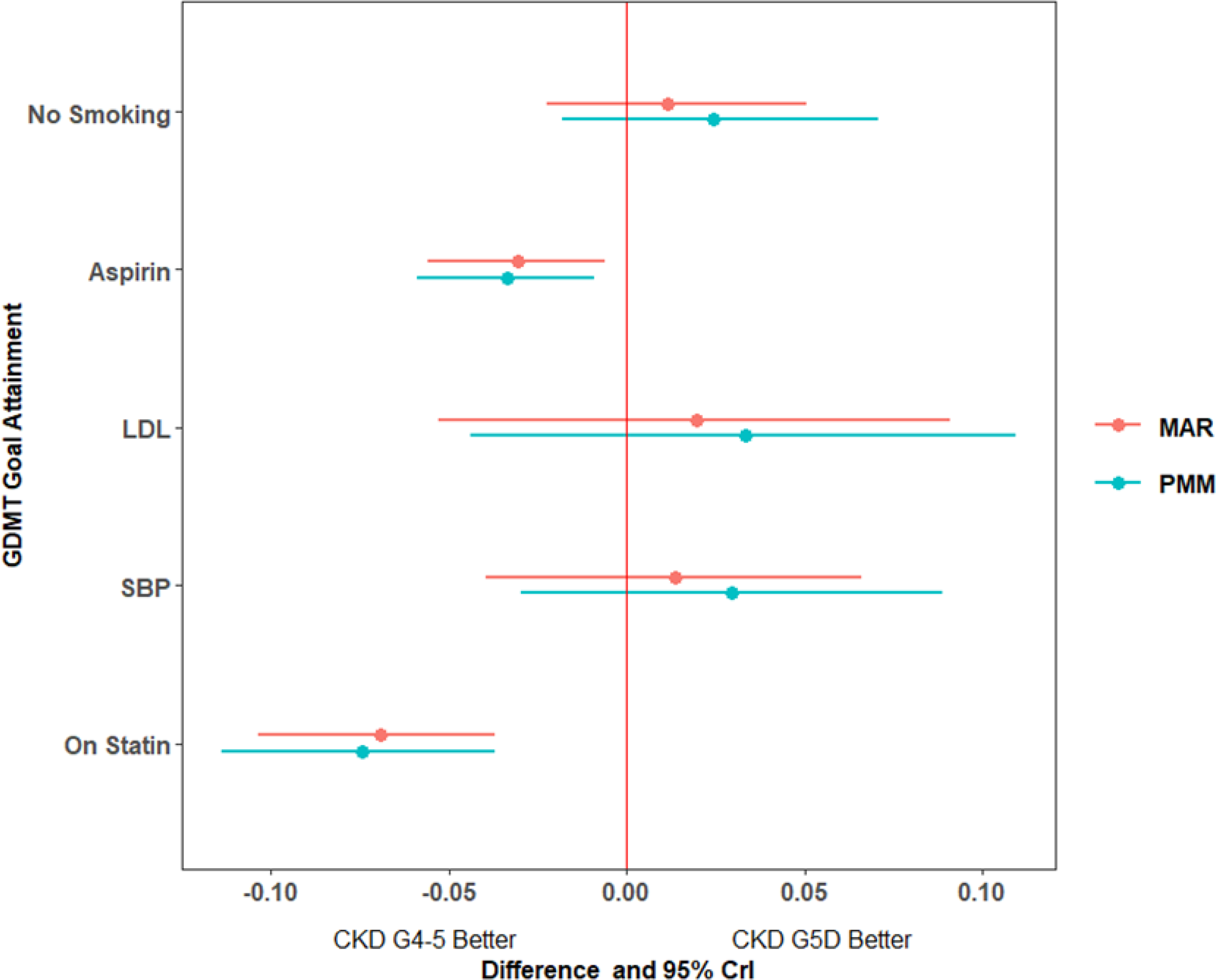
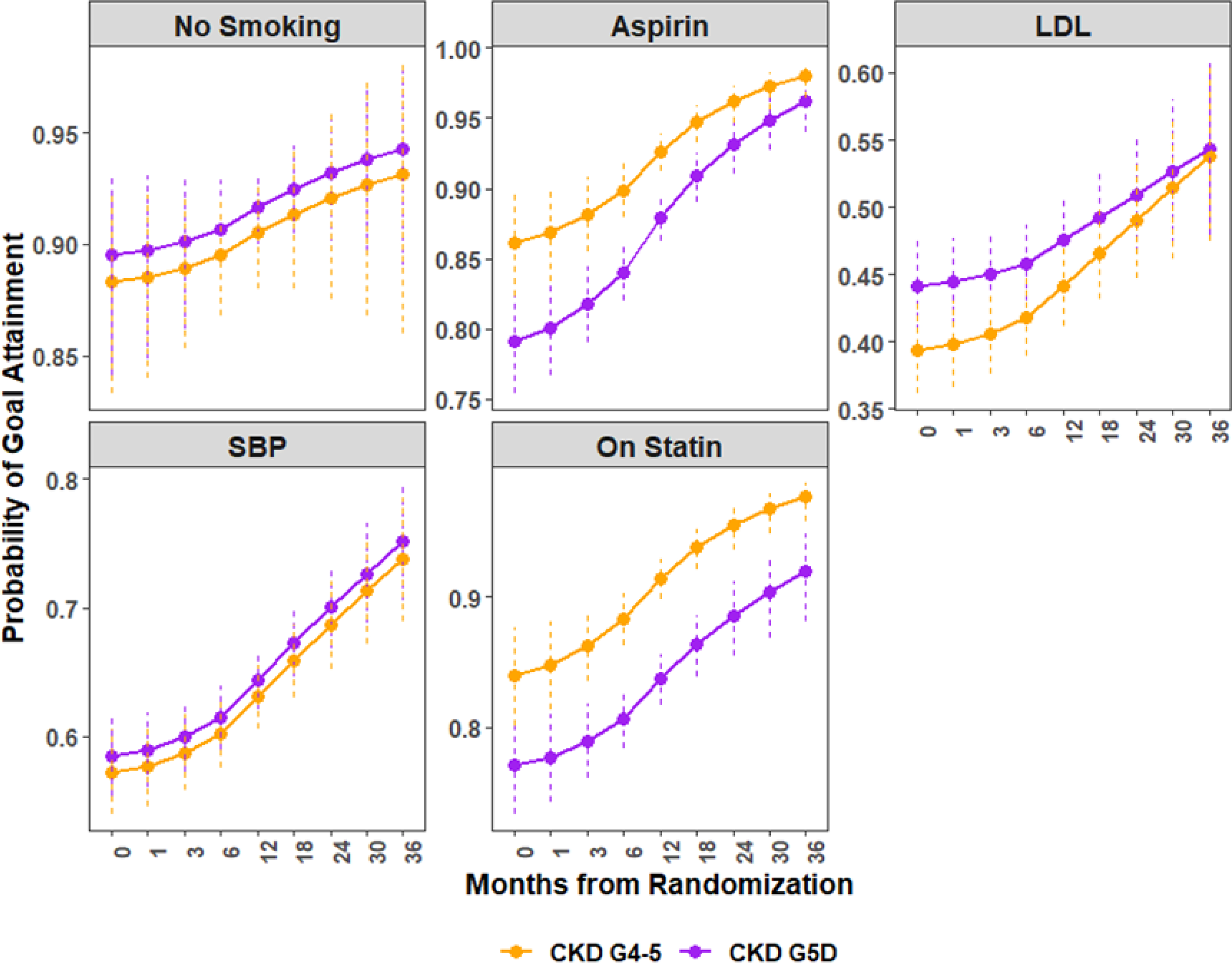
Methods: This was a subgroup analysis of ISCHEMIA-CKD (International Study of Comparative Health Effectiveness With Medical and Invasive Approaches-Chronic Kidney Disease) participants with CKD G4-5 or CKD G5D and moderate-to-severe myocardial ischemia on stress testing. Exposures included dialysis requirement at randomization and GDMT goal achievement during follow-up. The composite outcome was all-cause mortality or nonfatal myocardial infarction. Individual GDMT goal (smoking cessation, systolic blood pressure <140 mm Hg, low-density lipoprotein cholesterol <70 mg/dL, statin use, aspirin use) trajectory was modeled. Percentage point difference was estimated for each GDMT goal at 24 months between CKD G5D and CKD G4-5, and for association with key predictors. Probability of survival free from all-cause mortality or nonfatal myocardial infarction by GDMT goal achieved was assessed for CKD G5D versus CKD G4-5.
Results: A total of 415 CKD G5D and 362 CKD G4-5 participants were randomized. Participants with CKD G5D were less likely to receive statin (-6.9% [95% CI, -10.3% to -3.7%]) and aspirin therapy (-3.0% [95% CI, -5.6% to -0.6%]), with no difference in other GDMT goal attainment. Cumulative exposure to GDMT achieved during follow-up was associated with reduction in all-cause mortality or nonfatal myocardial infarction (hazard ratio, 0.88 [95% CI, 0.87-0.90]; per each GDMT goal attained over 60 days), irrespective of dialysis status.
Conclusions: CKD G5D participants received statin or aspirin therapy less often. Cumulative exposure to GDMT goals achieved was associated with lower incidence of all-cause mortality or nonfatal myocardial infarction in participants with advanced CKD and chronic coronary disease, regardless of dialysis status.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT01985360.
Keywords: cardiovascular diseases; clinical trial; kidney; lipoproteins; secondary prevention.
Figures
Similar articles
-
Attainment of Guideline-Directed Medical Treatment in Stable Ischemic Heart Disease Patients With and Without Chronic Kidney Disease.Cardiovasc Drugs Ther. 2019 Aug;33(4):443-451. doi: 10.1007/s10557-019-06883-z. Cardiovasc Drugs Ther. 2019. PMID: 31123935
-
Dialysis Initiation in Patients With Chronic Coronary Disease and Advanced Chronic Kidney Disease in ISCHEMIA-CKD.J Am Heart Assoc. 2022 Mar 15;11(6):e022003. doi: 10.1161/JAHA.121.022003. Epub 2022 Mar 9. J Am Heart Assoc. 2022. PMID: 35261290 Free PMC article. Clinical Trial.
-
Cardiovascular and Renal Implications of Myocardial Infarction in the ISCHEMIA-CKD Trial.Circ Cardiovasc Interv. 2022 Aug;15(8):e012103. doi: 10.1161/CIRCINTERVENTIONS.122.012103. Epub 2022 Aug 16. Circ Cardiovasc Interv. 2022. PMID: 35973009 Free PMC article. Clinical Trial.
-
Effects of statins on lipid profile in chronic kidney disease patients: a meta-analysis of randomized controlled trials.Curr Med Res Opin. 2013 May;29(5):435-51. doi: 10.1185/03007995.2013.779237. Epub 2013 Mar 11. Curr Med Res Opin. 2013. PMID: 23427811 Review.
-
Statins for treatment of dyslipidemia in chronic kidney disease.Perit Dial Int. 2006 Sep-Oct;26(5):523-39. Perit Dial Int. 2006. PMID: 16973506 Review.
Cited by
-
Contemporary secondary prevention in survivors of ST-elevation myocardial infarction with and without chronic kidney disease: a retrospective analysis.Clin Kidney J. 2023 Sep 4;16(11):1947-1956. doi: 10.1093/ckj/sfad219. eCollection 2023 Nov. Clin Kidney J. 2023. PMID: 37915929 Free PMC article.
-
Contemporary in-hospital and long-term prognosis of patients with acute ST-elevation myocardial infarction depending on renal function: a retrospective analysis.BMC Cardiovasc Disord. 2023 Feb 2;23(1):62. doi: 10.1186/s12872-023-03084-3. BMC Cardiovasc Disord. 2023. PMID: 36732721 Free PMC article.
-
Body Mass Index and Clinical and Health Status Outcomes in Chronic Coronary Disease and Advanced Kidney Disease in the ISCHEMIA-CKD Trial.Am J Med. 2024 Feb;137(2):163-171.e24. doi: 10.1016/j.amjmed.2023.10.024. Epub 2023 Nov 3. Am J Med. 2024. PMID: 37925061 Free PMC article.
References
-
- Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377:2181–2192. - PMC - PubMed
-
- Herrington WG, Emberson J, Mihaylova B, Blackwell L, Reith C, Solbu MD, Mark PB, Fellström B, Jardine AG, Wanner C, et al. Impact of renal function on the effects of LDL cholesterol lowering with statin-based regimens: a meta-analysis of individual participant data from 28 randomised trials. Lancet Diabetes Endocrinol. 2016;4:829–839. - PubMed
-
- Malhotra R, Nguyen HA, Benavente O, Mete M, Howard BV., Mant J, Odden MC, Peralta CA, Cheung AK, Nadkarni GN, et al. Association between more intensive vs less intensive blood pressure lowering and risk of mortality in chronic kidney disease stages 3 to 5: A systematic review and meta-analysis. JAMA Internal Medicine. 2017;177:1498–1505. - PMC - PubMed
-
- Der Mesropian PJ, Shaikh G, Cordero Torres E, Bilal A, Mathew RO. Antihypertensive therapy in nondiabetic chronic kidney disease: a review and update. Journal of the American Society of Hypertension. 2018;12:154–181. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
