

Artificial intelligence-based model for COVID-19 prognosis incorporating chest radiographs and clinical data; a retrospective model development and validation study
- PMID: 36193755
- PMCID: PMC9733620
- DOI: 10.1259/bjr.20220058
Artificial intelligence-based model for COVID-19 prognosis incorporating chest radiographs and clinical data; a retrospective model development and validation study
Abstract
Objectives: The purpose of this study was to develop an artificial intelligence-based model to prognosticate COVID-19 patients at admission by combining clinical data and chest radiographs.
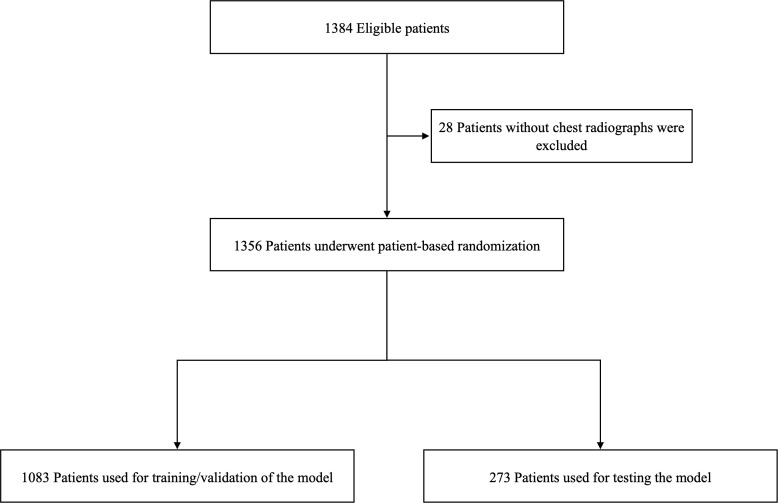
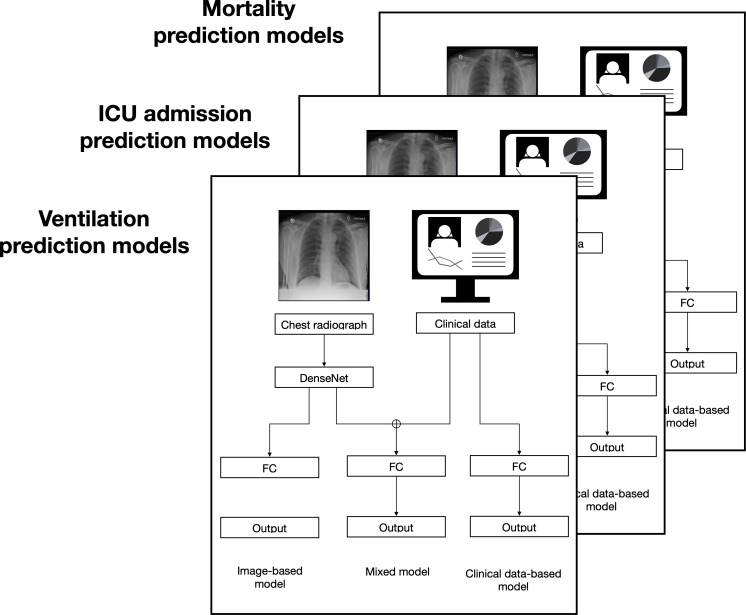
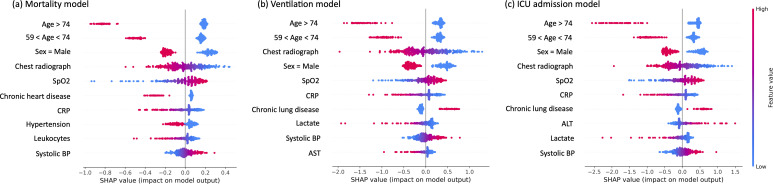
Methods: This retrospective study used the Stony Brook University COVID-19 dataset of 1384 inpatients. After exclusions, 1356 patients were randomly divided into training (1083) and test datasets (273). We implemented three artificial intelligence models, which classified mortality, ICU admission, or ventilation risk. Each model had three submodels with different inputs: clinical data, chest radiographs, and both. We showed the importance of the variables using SHapley Additive exPlanations (SHAP) values.
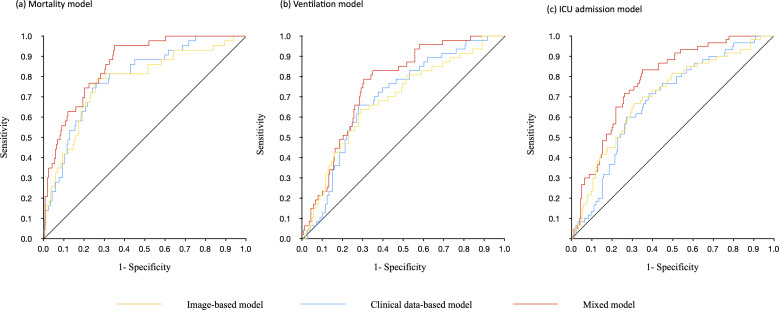
Results: The mortality prediction model was best overall with area under the curve, sensitivity, specificity, and accuracy of 0.79 (0.72-0.86), 0.74 (0.68-0.79), 0.77 (0.61-0.88), and 0.74 (0.69-0.79) for the clinical data-based model; 0.77 (0.69-0.85), 0.67 (0.61-0.73), 0.81 (0.67-0.92), 0.70 (0.64-0.75) for the image-based model, and 0.86 (0.81-0.91), 0.76 (0.70-0.81), 0.77 (0.61-0.88), 0.76 (0.70-0.81) for the mixed model. The mixed model had the best performance (p value < 0.05). The radiographs ranked fourth for prognostication overall, and first of the inpatient tests assessed.
Conclusions: These results suggest that prognosis models become more accurate if AI-derived chest radiograph features and clinical data are used together.
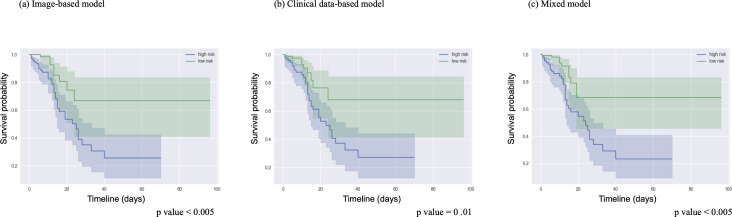
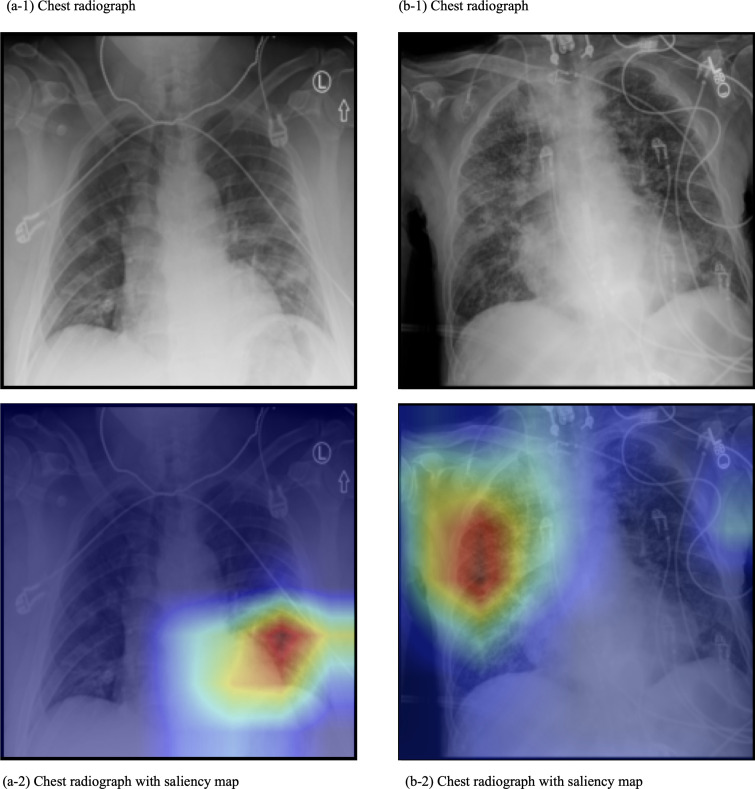
Advances in knowledge: This AI model evaluates chest radiographs together with clinical data in order to classify patients as having high or low mortality risk. This work shows that chest radiographs taken at admission have significant COVID-19 prognostic information compared to clinical data other than age and sex.
Figures
References
-
- WHO . Weekly epidemiological update—16 november 2021 . Available from : https://www.who.int/publications/m/item/weekly-epidemiological-update-on... ( accessed 16 Nov 2021 )
-
- Piva S, Filippini M, Turla F, Cattaneo S, Margola A, De Fulviis S, et al. . Clinical presentation and initial management critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in Brescia, Italy . J Crit Care 2020. ; 58 : 29 – 33 : S0883-9441(20)30547-5 . doi: 10.1016/j.jcrc.2020.04.004 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
