

Management of pediatric dialysis and kidney transplant patients after natural or man-made disasters
- PMID: 36194369
- PMCID: PMC9529603
- DOI: 10.1007/s00467-022-05734-8
Management of pediatric dialysis and kidney transplant patients after natural or man-made disasters
Abstract
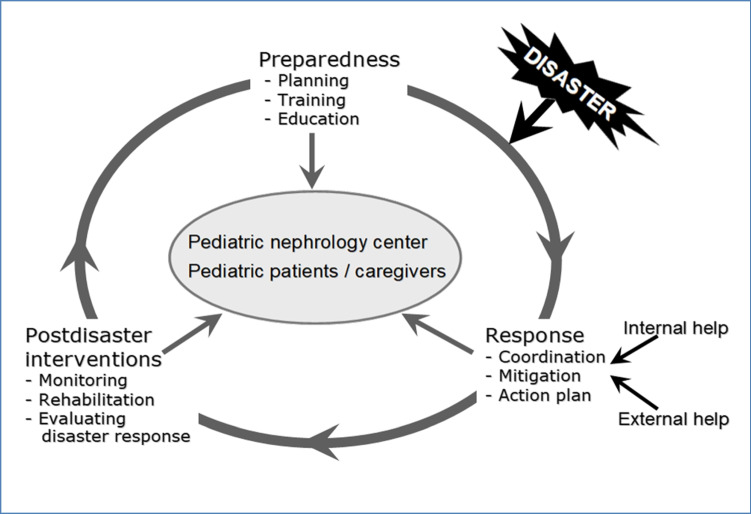
Pediatric patients on kidney replacement therapy (KRT) are among the most vulnerable during large-scale disasters, either natural or man-made. Hemodialysis (HD) treatments may be impossible because of structural damage and/or shortage of medical supplies, clean water, electricity, and healthcare professionals. Lack of peritoneal dialysis (PD) solutions and increased risk of infectious/non-infectious complications may make PD therapy challenging. Non-availability of immunosuppressants and increased risk of infections may result in graft loss and deaths of kidney transplant recipients. Measures to mitigate these risks must be considered before, during, and after the disaster including training of staff and patients/caregivers to cope with medical and logistic problems. Soon after a disaster, if the possibility of performing HD or PD is uncertain, patients should be directed to other centers, or the duration and/or number of HD sessions or the PD prescription adapted. In kidney transplant recipients, switching among immunosuppressants should be considered in case of non-availability of the medications. Post-disaster interventions target treating neglected physical and mental problems and also improving social challenges. All problems experienced by pediatric KRT patients living in the affected area are applicable to displaced patients who may also face extra risks during their travel and also at their destination. The need for additional local, national, and international help and support of non-governmental organizations must be anticipated and sought in a timely manner.
Keywords: Children; Dialysis; Kidney replacement therapy; Kidney transplant; Man-made disasters; Natural disasters; Nephrology.
© 2022. The Author(s), under exclusive licence to International Pediatric Nephrology Association.
Figures
References
-
- WHO/EHA (2002) Disasters & emergencies. Definitions. https://apps.who.int/disasters/repo/7656.pdf. Accessed 4 June 2022
-
- The United Nations International Strategy for Disaster Reduction (UNISDR) (2009) Disaster risk reduction. https://www.unisdr.org/files/7817_UNISDRTerminologyEnglish.pdf. Accessed 4 June 2022
-
- Al-Jazairi AF (2017) Disasters and disaster medicine. https://www.intechopen.com/chapters/58936. Accessed 4 June 2022
-
- Bodas M, Kirsch TD, Peleg K (2020) Top hazards approach – rethinking the appropriateness of the All-Hazards approach in disaster risk management. https://www.sciencedirect.com/science/article/abs/pii/S2212420919316358. Accessed 25 Aug 2022
-
- Sever MS, Vanholder R, Luyckx V, Eckardt KU, Kolesnyk M, Wiecek A, Pawlowicz-Szlarska E, Gallego D, Shroff R, Skoberne A, Nistor I, Sekkarie M, Ivanov D, Noruisiene E, Tuglular S, Renal Disaster Relief Task Force of the ERA Armed conflicts and kidney patients: a consensus statement from the renal disaster relief task force of the ERA. Nephrol Dial Transplant. 2022 doi: 10.1093/ndt/gfac247. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
