

Skeletal Muscle Adiposity and Lung Function Trajectory in the Severe Asthma Research Program
- PMID: 36194556
- PMCID: PMC9940151
- DOI: 10.1164/rccm.202203-0597OC
Skeletal Muscle Adiposity and Lung Function Trajectory in the Severe Asthma Research Program
Abstract
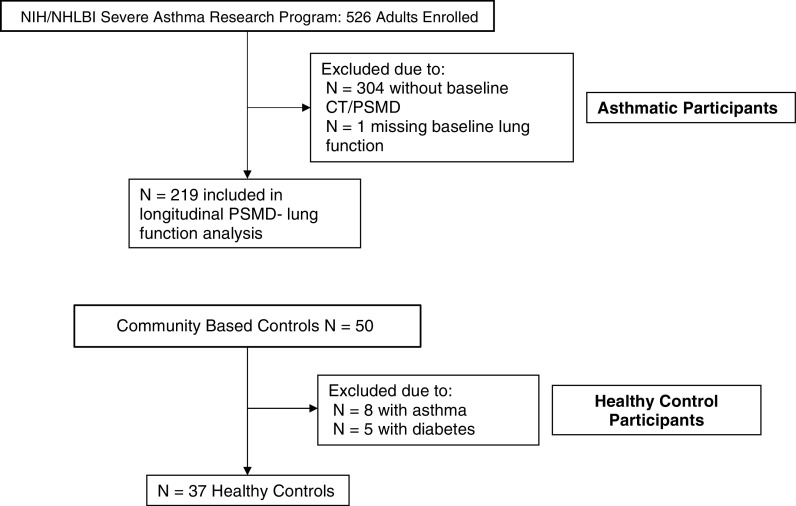
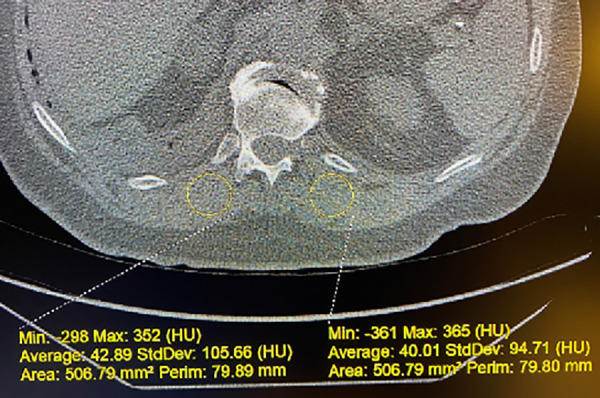
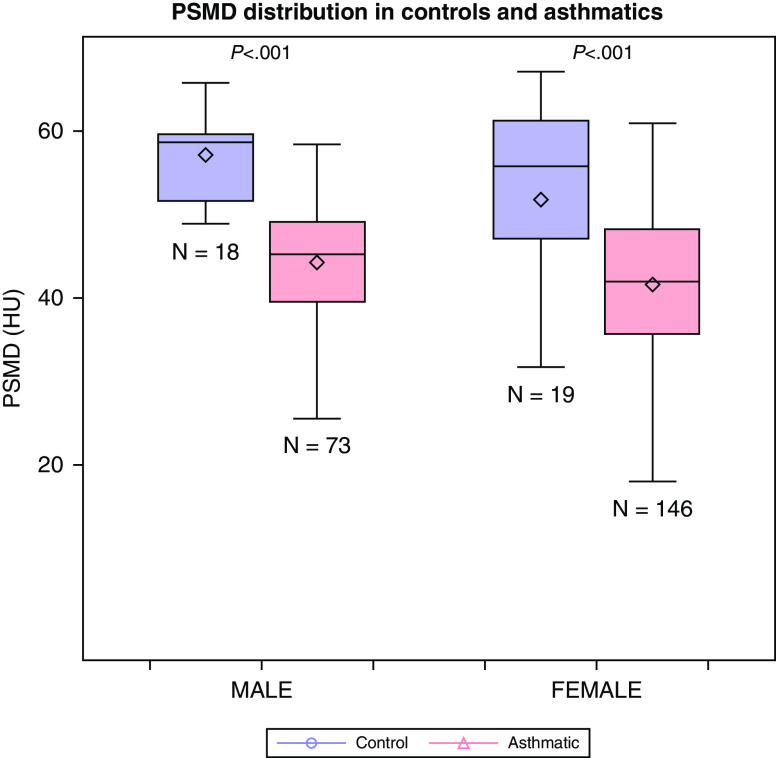
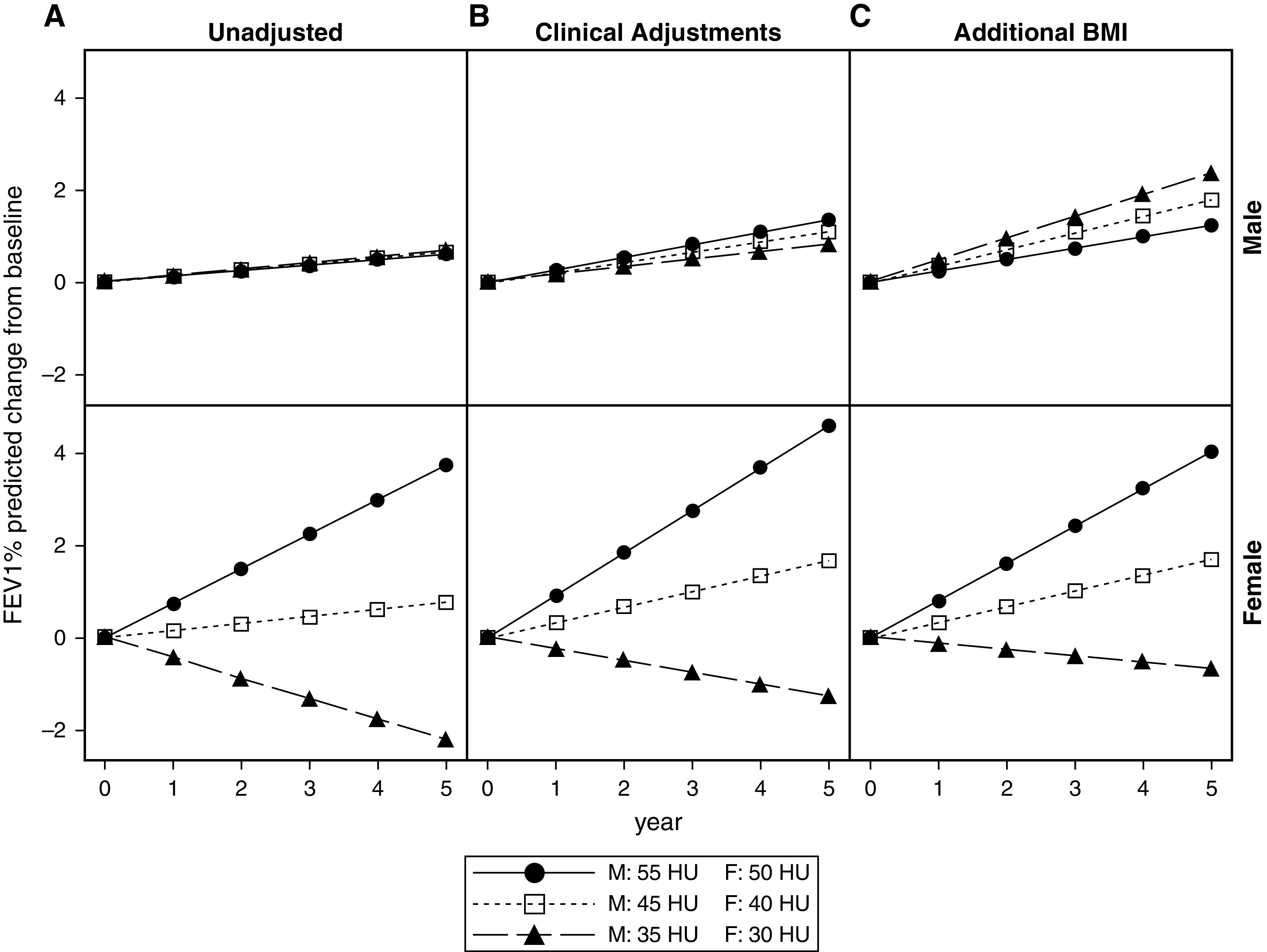
Rationale: Extrapulmonary manifestations of asthma, including fatty infiltration in tissues, may reflect systemic inflammation and influence lung function and disease severity. Objectives: To determine if skeletal muscle adiposity predicts lung function trajectory in asthma. Methods: Adult SARP III (Severe Asthma Research Program III) participants with baseline computed tomography imaging and longitudinal postbronchodilator FEV1% predicted (median follow-up 5 years [1,132 person-years]) were evaluated. The mean of left and right paraspinous muscle density (PSMD) at the 12th thoracic vertebral body was calculated (Hounsfield units [HU]). Lower PSMD reflects higher muscle adiposity. We derived PSMD reference ranges from healthy control subjects without asthma. A linear multivariable mixed-effects model was constructed to evaluate associations of baseline PSMD and lung function trajectory stratified by sex. Measurements and Main Results: Participants included 219 with asthma (67% women; mean [SD] body mass index, 32.3 [8.8] kg/m2) and 37 control subjects (51% women; mean [SD] body mass index, 26.3 [4.7] kg/m2). Participants with asthma had lower adjusted PSMD than control subjects (42.2 vs. 55.8 HU; P < 0.001). In adjusted models, PSMD predicted lung function trajectory in women with asthma (β = -0.47 Δ slope per 10-HU decrease; P = 0.03) but not men (β = 0.11 Δ slope per 10-HU decrease; P = 0.77). The highest PSMD tertile predicted a 2.9% improvement whereas the lowest tertile predicted a 1.8% decline in FEV1% predicted among women with asthma over 5 years. Conclusions: Participants with asthma have lower PSMD, reflecting greater muscle fat infiltration. Baseline PSMD predicted lung function decline among women with asthma but not men. These data support an important role of metabolic dysfunction in lung function decline.
Keywords: longitudinal lung function; muscle adiposity; severe asthma.
Figures
References
-
- Hansen EF, Phanareth K, Laursen LC, Kok-Jensen A, Dirksen A. Reversible and irreversible airflow obstruction as predictor of overall mortality in asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med . 1999;159:1267–1271. - PubMed
-
- Bai TR, Vonk JM, Postma DS, Boezen HM. Severe exacerbations predict excess lung function decline in asthma. Eur Respir J . 2007;30:452–456. - PubMed
-
- Coumou H, Westerhof GA, de Nijs SB, Zwinderman AH, Bel EH. Predictors of accelerated decline in lung function in adult-onset asthma. Eur Respir J . 2018;51:1701785. - PubMed
