

The different faces of metastatic melanoma in the gastrointestinal tract
- PMID: 36195726
- PMCID: PMC9532488
- DOI: 10.1186/s13244-022-01294-5
The different faces of metastatic melanoma in the gastrointestinal tract
Abstract
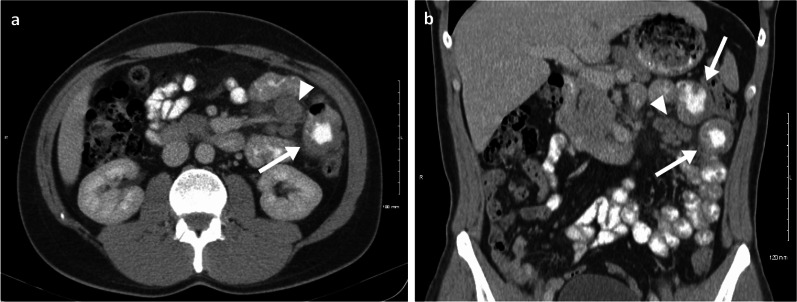
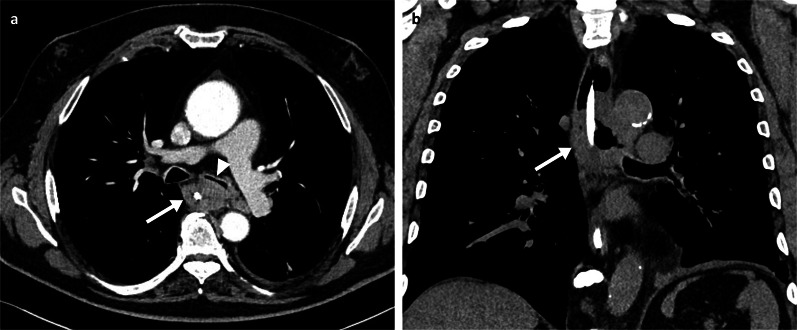
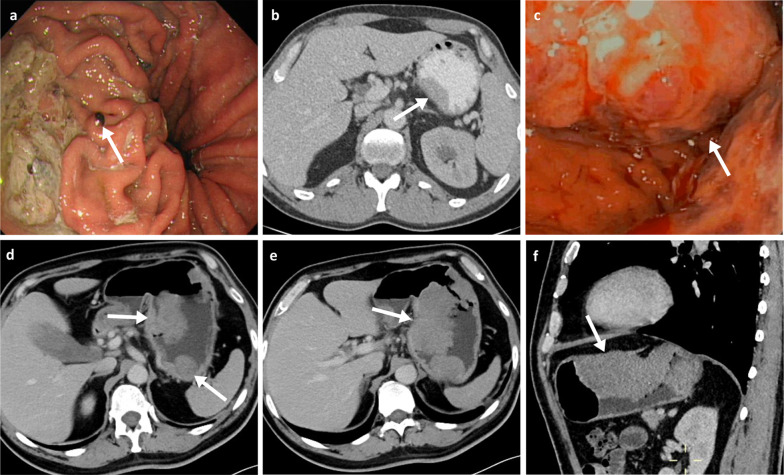
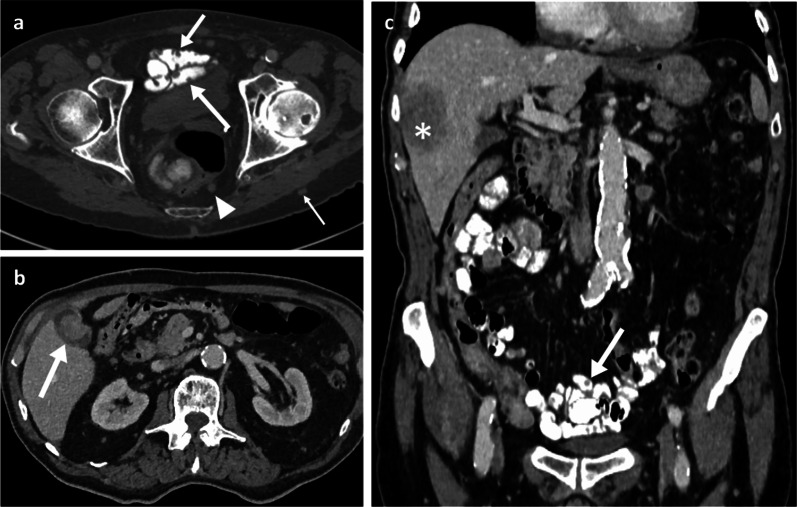
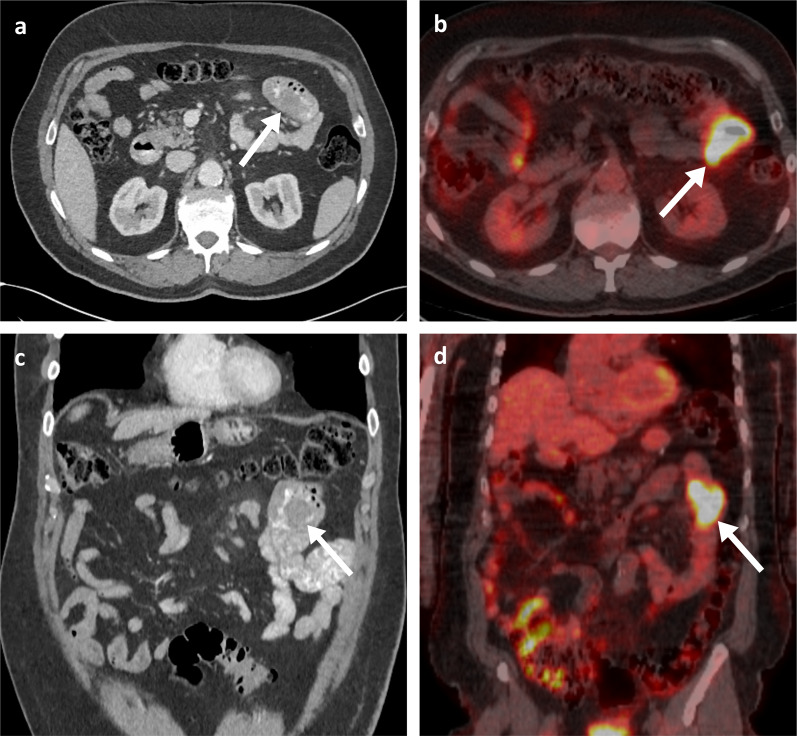
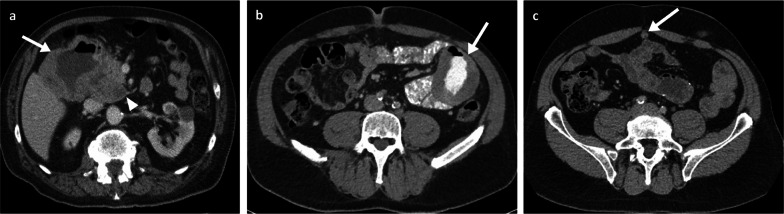
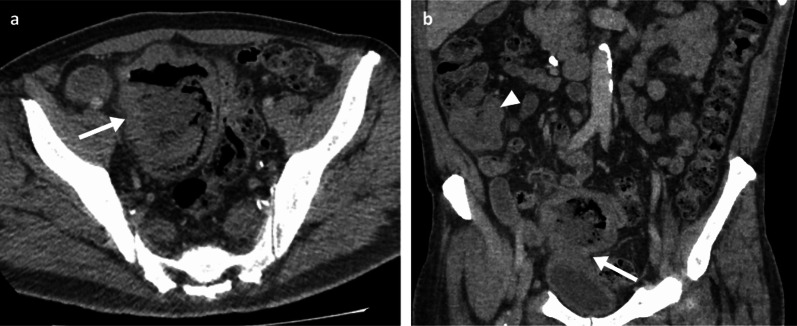
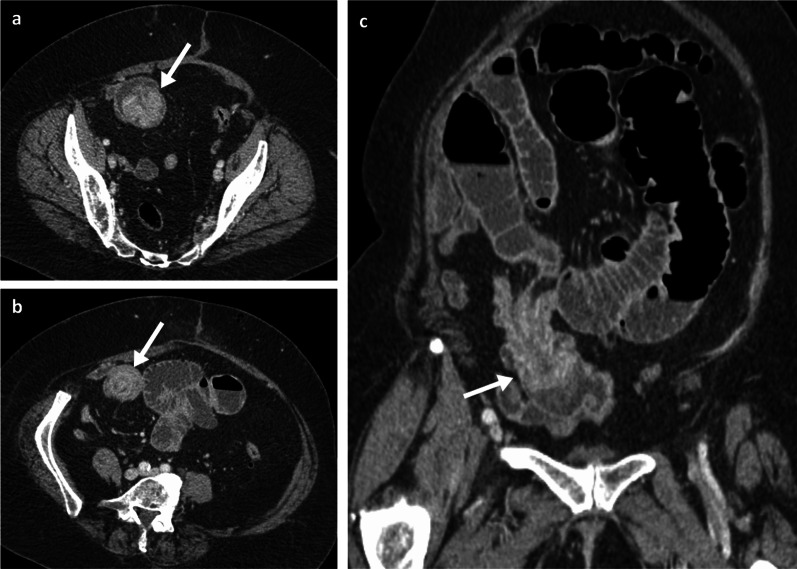
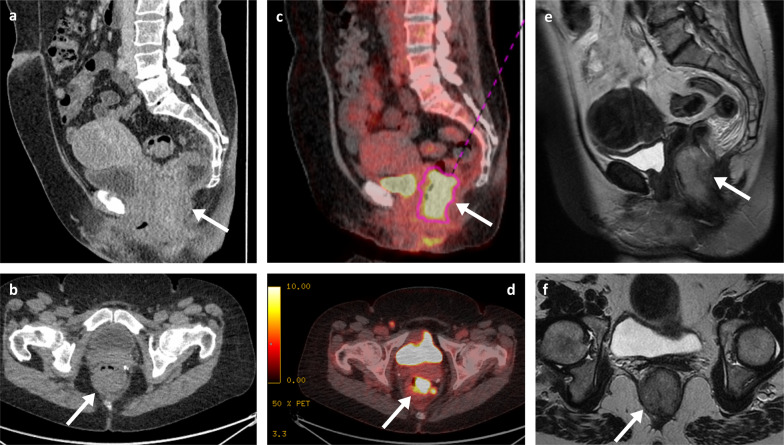
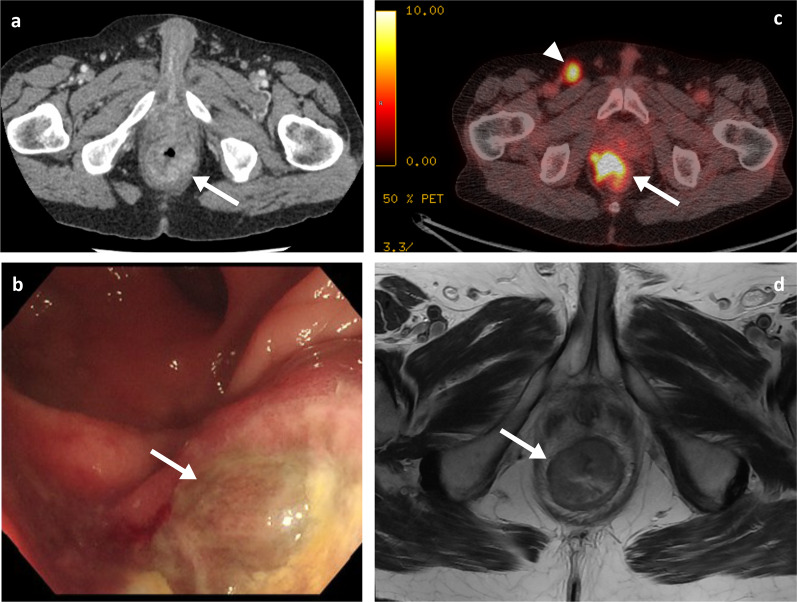
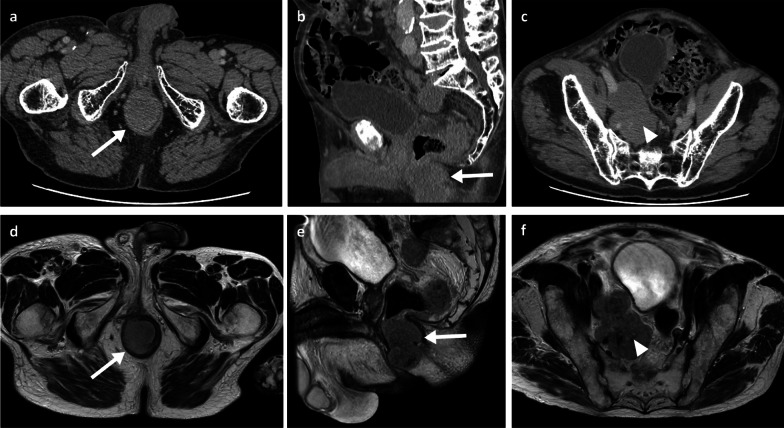
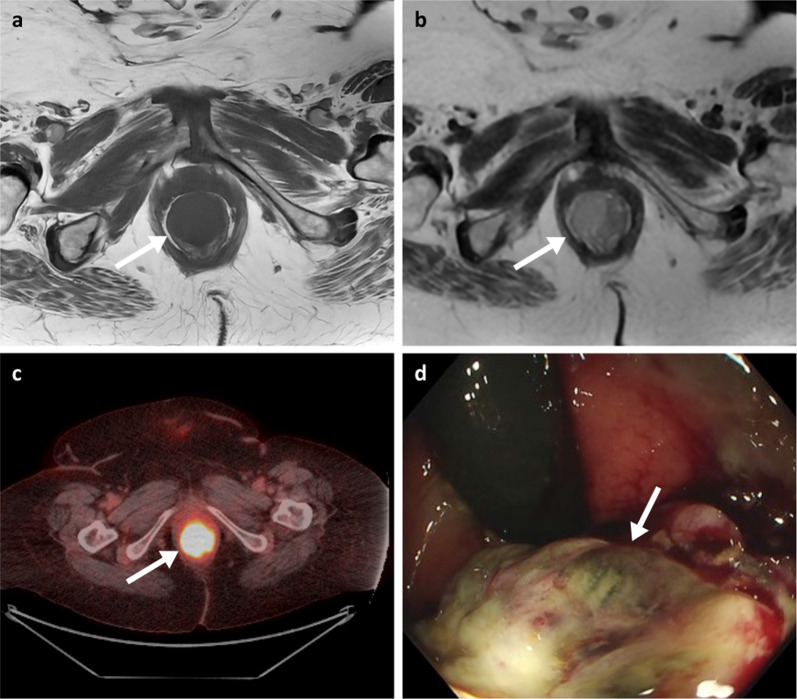
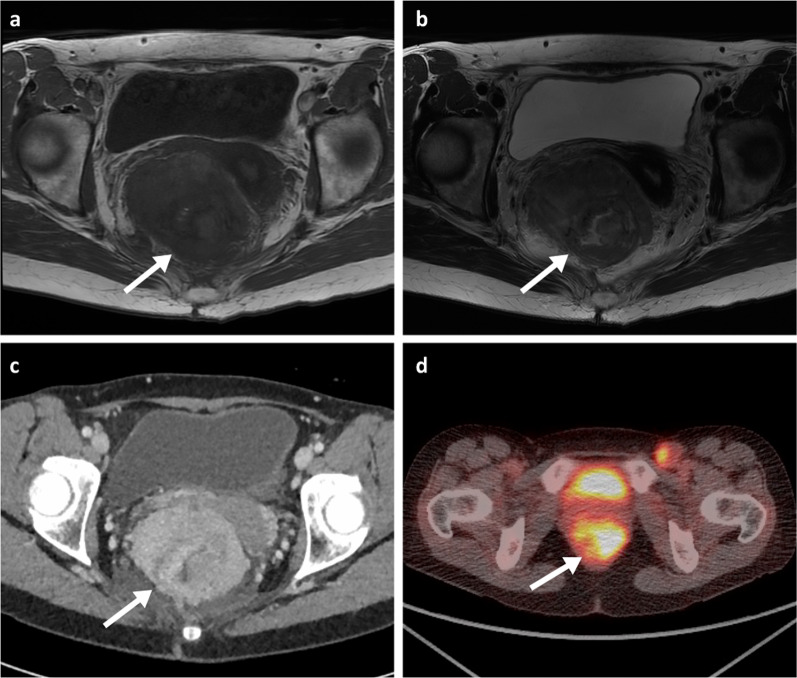
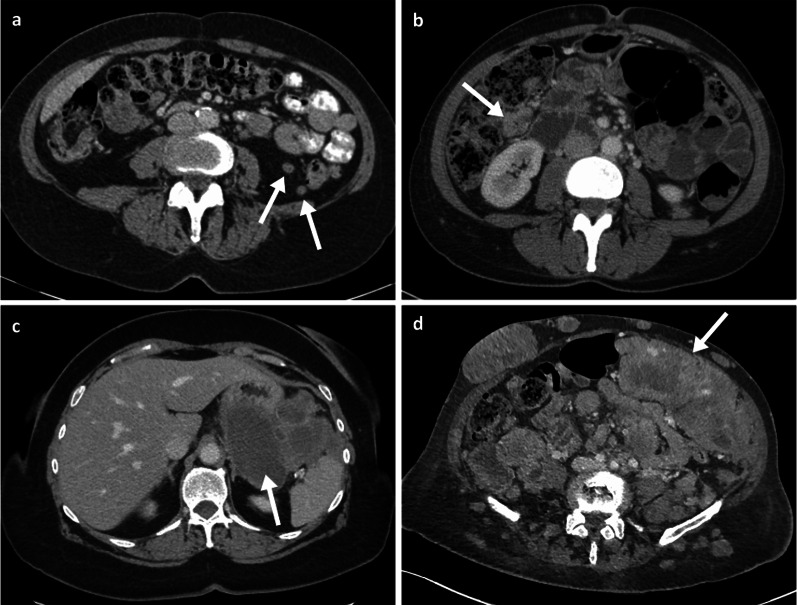
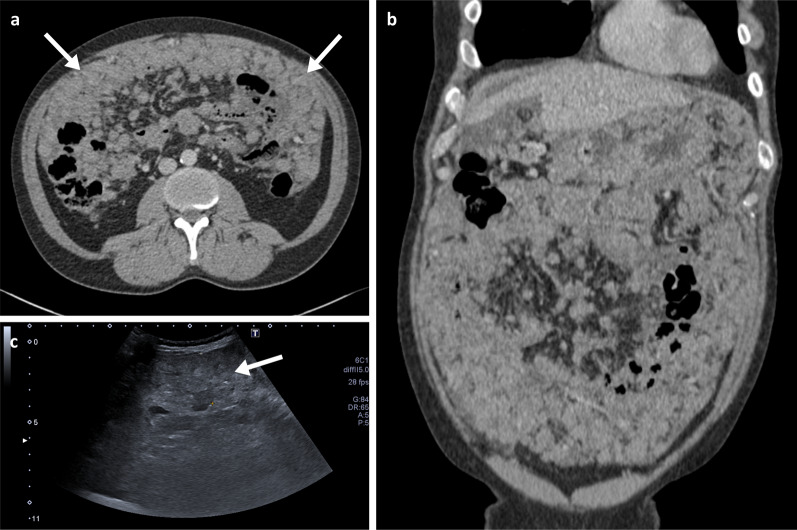
Melanoma is the most aggressive form of skin cancer, with tendency to spread to any organ of the human body, including the gastrointestinal tract (GIT). The diagnosis of metastases to the GIT can be difficult, as they may be clinically silent for somewhile and may occur years after the initial melanoma diagnosis. CT imaging remains the standard modality for staging and surveillance of melanoma patients, and in most cases, it will be the first imaging modality to identify GIT lesions. However, interpretation of CT studies in patients with melanoma can be challenging as lesions may be subtle and random in distribution, as well as sometimes mimicking other conditions. Even so, early diagnosis of GIT metastases is critical to avoid emergency hospitalisations, whilst surgical intervention can be curative in some cases. In this review, we illustrate the various imaging presentations of melanoma metastases within the GIT, discuss the clinical aspects and offer advice on investigation and management. We offer tips intended to aid radiologists in their diagnostic skills and interpretation of melanoma imaging scans.
Keywords: Gastrointestinal tract; Magnetic resonance imaging; Melanoma; Metastases; Tomography (X-ray computed).
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- *SEER*Explorer: An Interactive Website for SEER Cancer Statistics. 7/4/22. https://seer.cancer.gov/explorer.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
