

Post-mortem examination of high mortality in patients with heart failure and atrial fibrillation
- PMID: 36195871
- PMCID: PMC9533594
- DOI: 10.1186/s12916-022-02533-8
Post-mortem examination of high mortality in patients with heart failure and atrial fibrillation
Abstract
Background: The prevalence of combined heart failure (HF) and atrial fibrillation (AF) is rising, and these patients suffer from high rates of mortality. This study aims to provide robust data on factors associated with death, uniquely supported by post-mortem examination.
Methods: A retrospective cohort study of hospitalized adults with a clinical diagnosis of HF and AF at a tertiary centre in Romania between 2014 and 2017. A standardized post-mortem examination was performed where death occurred within 24 h of admission, when the cause of death was not clear or by physician request. National records were used to collect mortality data, subsequently categorized and analysed as HF-related death, vascular death and non-cardiovascular death using Cox proportional hazards regression.
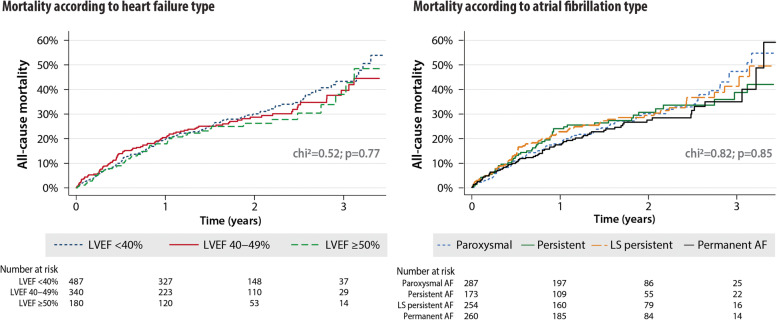
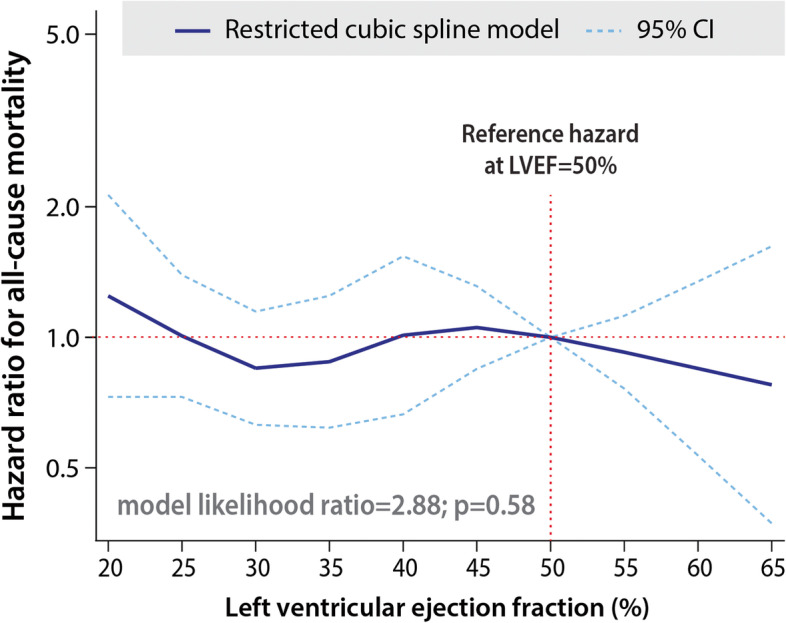
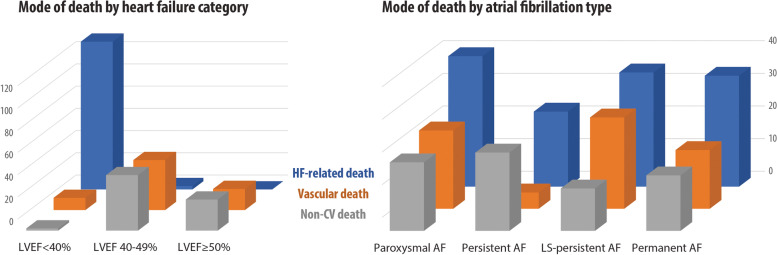
Results: A total of 1009 consecutive patients with a mean age of 73 ± 11 years, 47% women, NYHA class 3.0 ± 0.9, left ventricular ejection fraction (LVEF) 40.1 ± 11.0% and 100% anticoagulated were followed up for 1.5 ± 0.9 years. A total of 291 (29%) died, with post-mortems performed on 186 (64%). Baseline factors associated with mortality were dependent on the cause of death. HF-related death in 136 (47%) was associated with higher NYHA class (hazard ratio [HR] 2.45 per one class increase, 95% CI 1.73-3.46; p < 0.001) and lower LVEF (0.95 per 1% increase, 0.93-0.97; p < 0.001). Vascular death occurred in 75 (26%) and was associated with hypertension (HR 2.83, 1.36-5.90; p = 0.005) and higher LVEF (1.08 per 1% increase, 1.05-1.11; p < 0.001). Non-cardiovascular death in 80 (28%) was associated with clinical obesity (HR 2.20, 1.21-4.00; p = 0.010) and higher LVEF (1.10 per 1% increase, 1.06-1.13; p < 0.001). Across all causes, there was no relationship between mortality and AF type (p = 0.77), HF type (p = 0.85) or LVEF (p = 0.58).
Conclusions: Supported by post-mortem data, the cause of death in HF and AF patients is heterogeneous, and the relationships with typical markers of mortality are critically dependent on the mode of death. The poor prognosis in this group demands further attention to improve management beyond anticoagulation.
Keywords: Atrial fibrillation; Autopsy; Heart failure; Mortality; Post-mortem.
© 2022. The Author(s).
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form and declare the following: Otilia Tica received salary funding from the EU/EEPIA Innovative Medicines Initiative (BigData@Heart 116074) and Amomed Pharma, awarded to Professor Kotecha. Professor Kotecha reports grants from the National Institute for Health Research (NIHR CDF-2015–08-074 RATE-AF; NIHR HTA-130280 DaRe2THINK), the British Heart Foundation (PG/17/55/33087 and AA/18/2/34218), EU/EFPIA Innovative Medicines Initiative (BigData@Heart 116074), the European Society of Cardiology supported by educational grants from Boehringer Ingelheim/BMS-Pfizer Alliance/Bayer/Daiichi Sankyo/Boston Scientific, the NIHR/University of Oxford Biomedical Research Centre and British Heart Foundation/University of Birmingham Accelerator Award (STEEER-AF NCT04396418) and Amomed Pharma and IRCCS San Raffaele/Menarini (Beta-blockers in Heart Failure Collaborative Group NCT0083244), in addition to personal fees from Bayer (Advisory Board), AtriCure (Speaker fees), Amomed (Advisory Board), Protherics Medicines Development (Advisory Board) and Myokardia (Advisory Board). Dr. Ovidiu Tica, Dr. deBono, Professor Popescu and Professor Gkoutos declare that they have no competing interests. Dr. Bunting was the research fellow for the RATE-AF trial funded by the NIHR (NIHR CDF-2015–08-074) and has been awarded a grant from the University of Birmingham’s British Heart Foundation Accelerator Award (BHF AA/18/2/34218) and the British Heart Foundation Fellowship scheme (FS/CDRF/21/21032).
Figures
References
-
- Li X, Tse VC, Au-Doung LW, Wong ICK, Chan EW. The impact of ischaemic stroke on atrial fibrillation-related healthcare cost: a systematic review. Europace. 2017;19(6):937–947. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
