

Comparative clinical outcome following individualized follitropin delta dosing in Chinese women undergoing ovarian stimulation for in vitro fertilization /intracytoplasmic sperm injection
- PMID: 36195924
- PMCID: PMC9531501
- DOI: 10.1186/s12958-022-01016-y
Comparative clinical outcome following individualized follitropin delta dosing in Chinese women undergoing ovarian stimulation for in vitro fertilization /intracytoplasmic sperm injection
Abstract
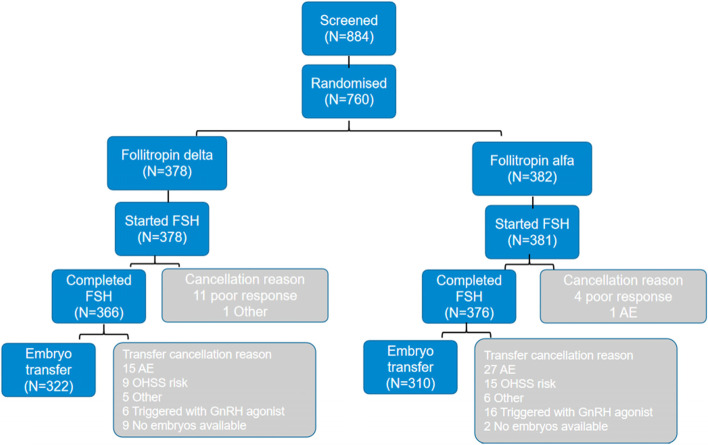
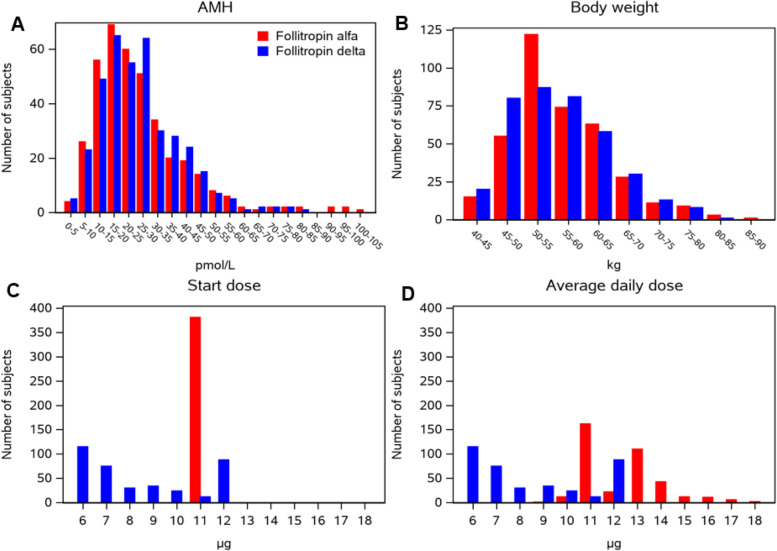
Background: To compare the efficacy and safety of follitropin delta in its individualized fixed-dose regimen with follitropin alfa in a conventional adjustable dosing regimen in Chinese women. METHODS: This was a subgroup analysis of the randomized, multi-center, assessor-blind, non-inferiority trial (GRAPE) including 759 Chinese women (aged 20-40 years) recruited in 16 reproductive medicine clinics in China. Women were randomized in a 1:1 ratio to be treated with either follitropin delta dose based on anti-Müllerian hormone (AMH) and body weight or conventional dosing with follitropin alfa following a gonadotropin-releasing hormone (GnRH) antagonist protocol. The primary outcome was ongoing pregnancy rate assessed 10-11 weeks after embryo transfer in the fresh cycle (non-inferiority margin -10.0%).
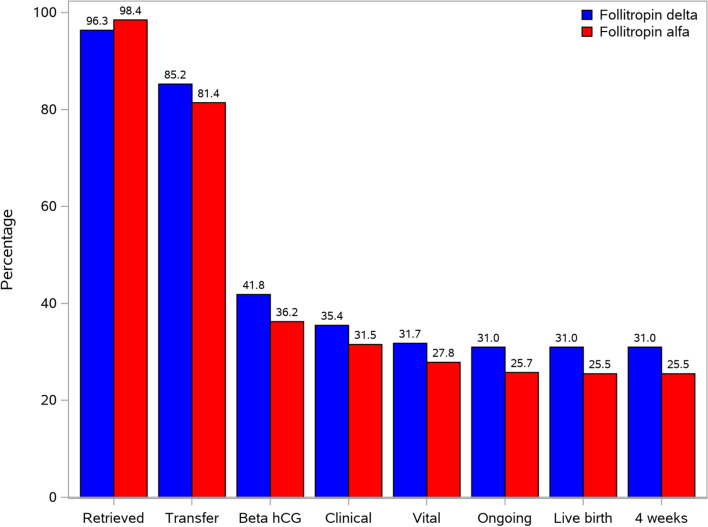
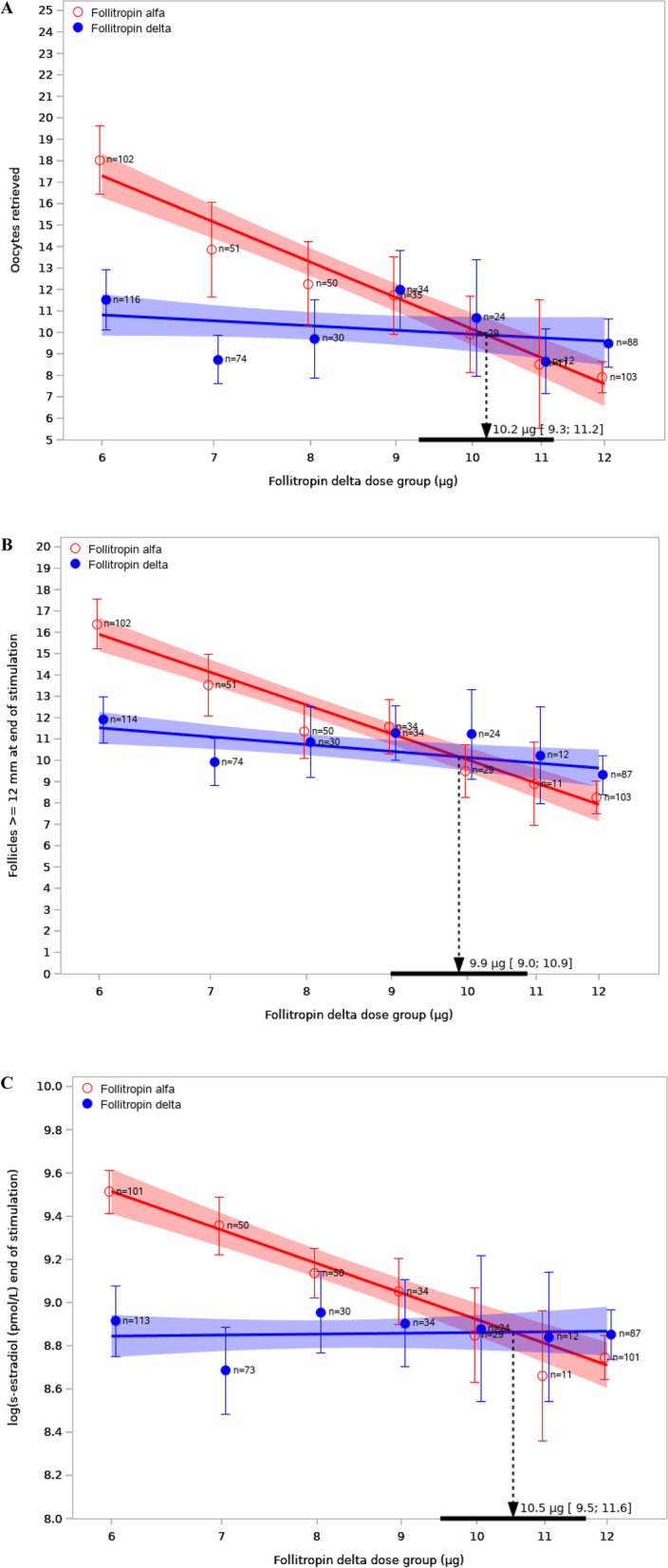
Results: 378 in the follitropin delta group and 381 in the follitropin alfa group were randomized and exposed. Non-inferiority was confirmed with respect to ongoing pregnancy with rates of 31.0% vs. 25.7% for follitropin delta compared to follitropin alfa, estimated mean difference of 5.1% (95% confidence interval (CI) -1.3% to 11.5%). The clinical pregnancy rate (35.4% vs. 31.5%, P = 0.239) and live birth rate (31.0% vs. 25.5%, P = 0.101) were comparable between the follitropin delta group and the follitropin alfa group. Overall, the individualized follitropin delta treatment resulted in fewer oocytes retrieved compared to follitropin alfa treatment (10.3 ± 6.2 vs. 12.5 ± 7.5, P < 0.001), which was mainly due to fewer oocytes (10.5 ± 6.4 vs. 13.9 ± 7.8) in women with AMH ≥ 15 pmol/L. Accordingly there was a lower incidence of early ovarian hyper-stimulation syndrome (OHSS) and/or preventive interventions (6.1% vs. 11.0%, P = 0.013). A daily follitropin delta dose of 10.2 µg (95% CI: 9.3-11.2 µg) was estimated to provide the same number of oocytes retrieved as a starting dose of 150 IU/d of follitropin alfa.
Conclusion: Follitropin delta in its individualized fixed-dose regimen showed similar efficacy and improved safety compared with follitropin alfa in a conventional adjustable dosing regimen in Chinese women.
Clinical trial registration number: NCT03296527.
Keywords: Algorithm; Dose equivalence; Follitropin delta; Individualized dosing; Ongoing pregnancy; Ovarian hyperstimulation syndrome.
© 2022. The Author(s).
Conflict of interest statement
Marie Goethberg and Bernadette Mannaerts are employees of Ferring Pharmaceuticals, Denmark. Wen Wu and Zugeng Zheng are employees of Ferring Pharmaceuticals, China. The other authors have stated explicitly that there are no conflicts of competing interests with the article.
Figures
References
-
- Nyboe Andersen A, Nelson SM, Fauser BC, García-Velasco JA, Klein BM, Arce JC, et al. Individualized versus conventional ovarian stimulation for in vitro fertilization: a multicenter, randomized, controlled, assessor-blinded, phase 3 noninferiority trial. Fertil Steril. 2017;107(387–96):e4. - PubMed
-
- Stormlund S, Sopa N, Zedeler A, Bogstad J, Prætorius L, Nielsen HS, et al. Freeze-all versus fresh blastocyst transfer strategy during in vitro fertilisation in women with regular menstrual cycles: multicentre randomised controlled trial. BMJ. 2020;370:m2519. doi: 10.1136/bmj.m2519. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
