

His-bundle Pacing as a Bailout Therapy for a Patient with Subclavian Stenosis and No Suitable Coronary Sinus Branch: A Double Whammy
- PMID: 36196239
- PMCID: PMC9521728
- DOI: 10.19102/icrm.2022.130902
His-bundle Pacing as a Bailout Therapy for a Patient with Subclavian Stenosis and No Suitable Coronary Sinus Branch: A Double Whammy
Abstract
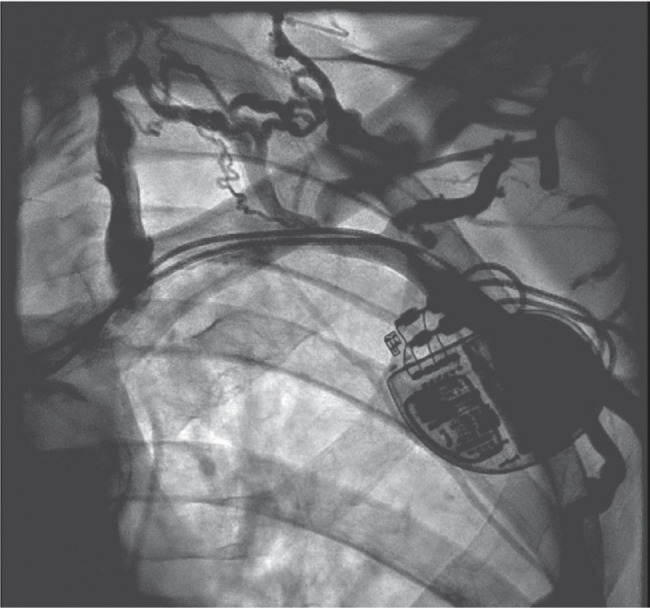
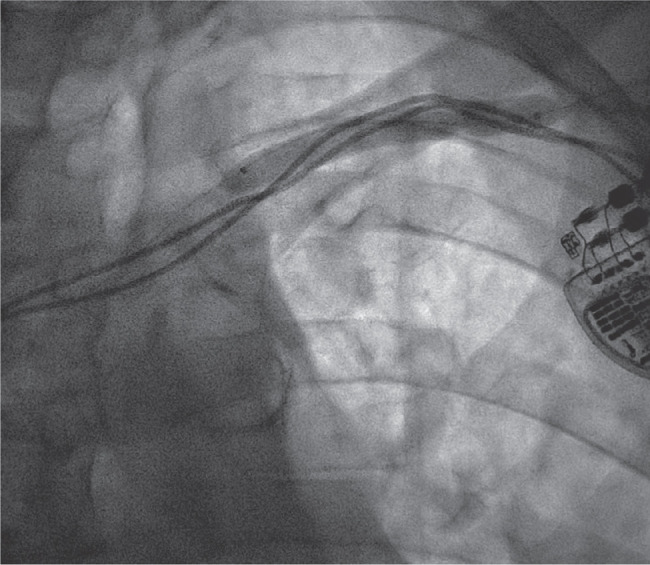
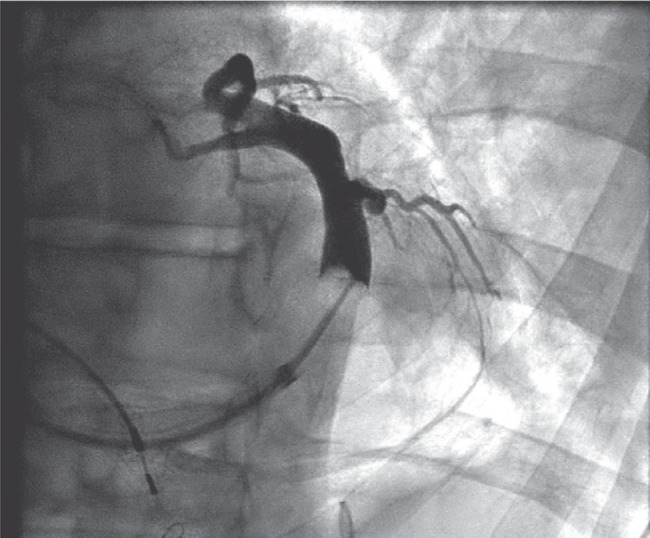
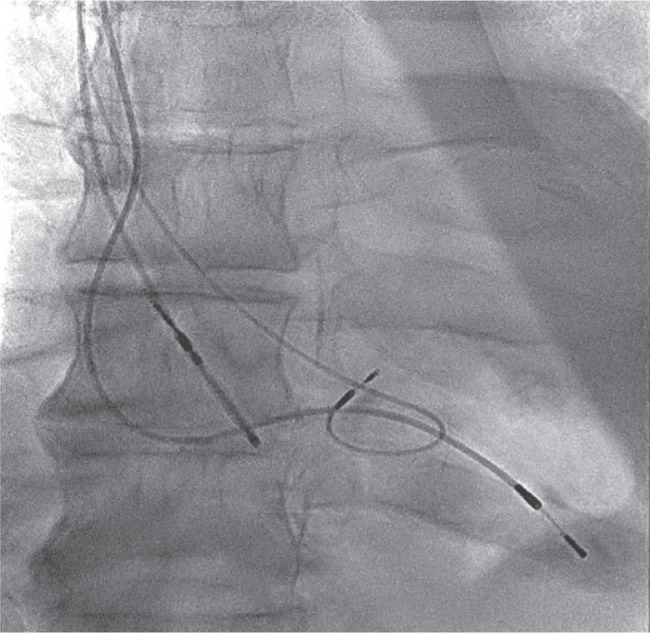
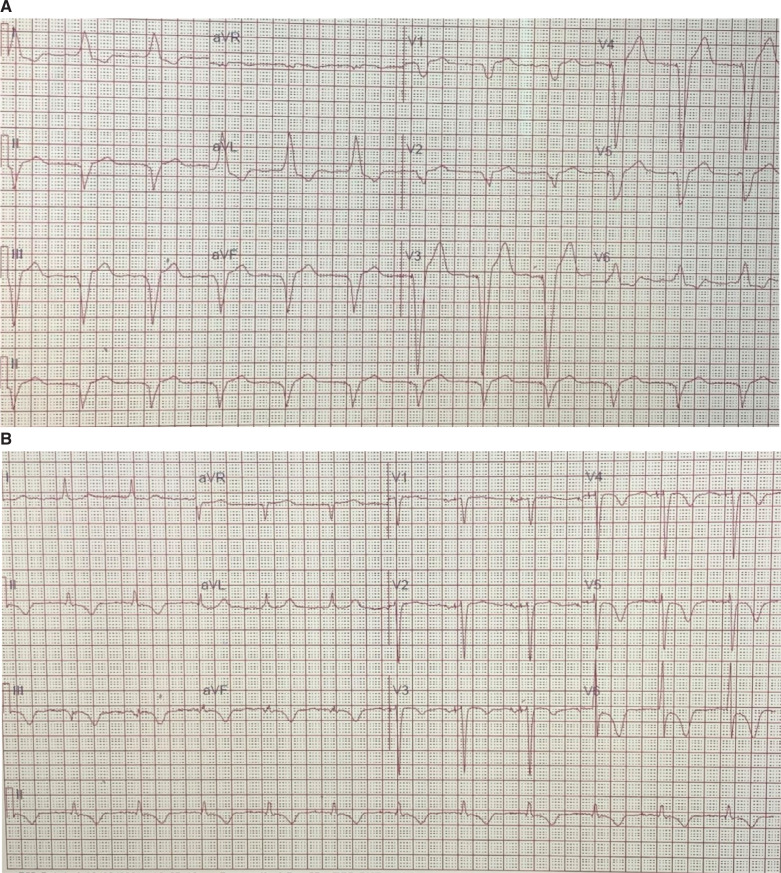
We present an interesting case of an 88-year-old man who was referred to our arrhythmia service for an upgrade of his dual-chamber pacemaker to a biventricular pacemaker for right ventricular pacing-induced cardiomyopathy. The patient was found to have stenosis of the left subclavian vein. Here, we describe the approach used to perform venoplasty in this patient. After venoplasty of the left subclavian vein, the patient did not have suitable coronary venous anatomy for deployment of the coronary sinus lead. Subsequently, a His lead was implanted. We achieved significant narrowing of the QRS with good thresholds and other lead parameters. Through this case report, we seek to present our approach of venoplasty in patients with occluded venous access for either an upgrade or a de novo implant.
Keywords: Cardiac resynchronization therapy; His pacing; subclavian stenosis.
Copyright: © 2022 Innovations in Cardiac Rhythm Management.
Conflict of interest statement
The authors report no conflicts of interest for the published content. No funding information was provided.
Figures
References
-
- Sticherling C, Chough SP, Baker RL, et al. Prevalence of central venous occlusion in patients with chronic defibrillator leads. Am Heart J. 2001;141(5):813–816. [CrossRef] [PubMed] - DOI - PubMed
-
- Oginosawa Y, Abe H, Nakashima Y. The incidence and risk factors for venous obstruction after implantation of transvenous pacing leads. Pacing Clin Electrophysiol. 2002;25(11):1605–1611. [CrossRef] [PubMed] - DOI - PubMed
-
- Worley SJ, Gohn DC, Pulliam RW, Raifsnider MA, Ebersole BI, Tuzi J. Subclavian venoplasty by the implanting physicians in 373 patients over 11 years. Heart Rhythm. 2011;8(4):526–533. [CrossRef] [PubMed] - DOI - PubMed
-
- Kusumoto FM, Schoenfeld MH, Wilkoff BL, et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503–e551. [CrossRef] [PubMed] - DOI - PubMed
-
- Marcial JM, Worley SJ. Venous system interventions for device implantation. Card Electrophysiol Clin. 2018;10(1):163–177. [CrossRef] [PubMed] - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources