

Glioblastoma - treatment and obstacles
- PMID: 36196416
- PMCID: PMC9521695
- DOI: 10.5603/RPOR.a2022.0076
Glioblastoma - treatment and obstacles
Abstract
Background: Glioblastoma is the most common and aggressive primary tumor in adults. A narrative review of all the relevant papers known was conducted.
Materials and methods: Reviews, clinical trials, and randomized controlled trials published from 1981 through September 2021 and written, or at least abstracted, in English were analyzed.
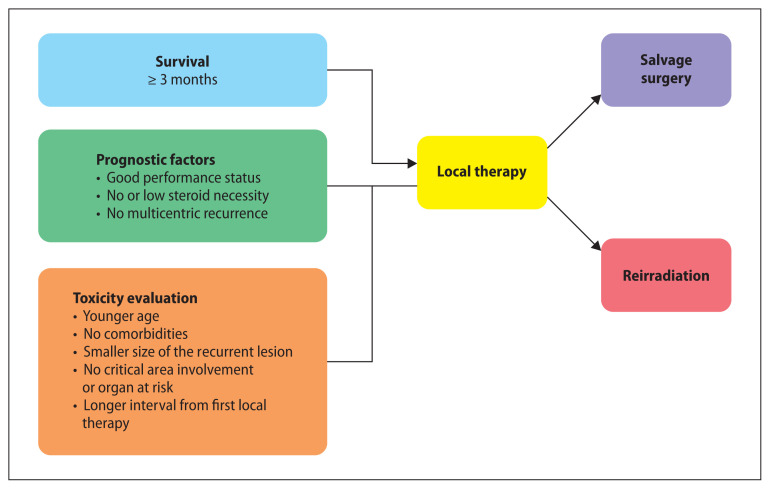
Results: The standard of care for glioblastoma is the maximum safe resection possible, followed by radiation therapy and concurrent temozolomide (TMZ) and daily TMZ and tumor treatment fields (TTFields) after irradiation. There is no evidence to date of the benefit of brachytherapy, radiosurgery (SRS), fractional stereotactic radiotherapy (FSRT), and hyperfractionated radiotherapy over conventional external beam radiation therapy (EBRT) for the primary tumor. The assessment of age and performance status before treatment in the elderly enables hypofractionated radiotherapy. The research of tumor molecular signatures contributes to the choice of the best-targeted drug therapy. In recurrent glioblastoma, it is necessary to balance the risks and benefits of re-radiation and association with bevacizumab. Solid data confirming the role of immunotherapy in the treatment of malignant glioma are still lacking.
Conclusions: Although the treatment of glioblastoma has evolved in terms of local control, mortality remains close to 12 months after diagnosis. To obtain better results and reduce recurrence, future research needs to investigate the frontiers of knowledge, such as the elucidation of the molecular mechanisms related to the tumor, the optimization of drugs to overcome the blood-brain barrier effectively, and the discovery of new therapies aimed at the heterogeneous profile of this neoplasm.
Keywords: glioblastoma; malignant glioma; radiation therapy; temozolomide.
© 2022 Greater Poland Cancer Centre.
Conflict of interest statement
Conflicts of interest None declared.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources