

Testosterone and long pulse width stimulation (TLPS) for denervated muscles after spinal cord injury: a study protocol of randomised clinical trial
- PMID: 36198461
- PMCID: PMC9535184
- DOI: 10.1136/bmjopen-2022-064748
Testosterone and long pulse width stimulation (TLPS) for denervated muscles after spinal cord injury: a study protocol of randomised clinical trial
Abstract
Introduction: Long pulse width stimulation (LPWS; 120-150 ms) has the potential to stimulate denervated muscles and to restore muscle size in denervated people with spinal cord injury (SCI). We will determine if testosterone treatment (TT)+LPWS would increase skeletal muscle size, leg lean mass and improve overall metabolic health in persons with SCI with denervation. We hypothesise that the 1-year TT+LPWS will upregulate protein synthesis pathways, downregulate protein degradation pathways and increase overall mitochondrial health.
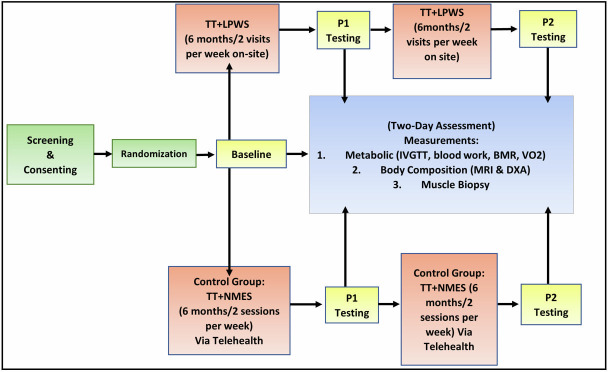
Methods and analysis: Twenty-four male participants (aged 18-70 years with chronic SCI) with denervation of both knee extensor muscles and tolerance to the LPWS paradigm will be randomised into either TT+neuromuscular electrical stimulation via telehealth or TT+LPWS. The training sessions will be twice weekly for 1 year. Measurements will be conducted 1 week prior training (baseline; week 0), 6 months following training (postintervention 1) and 1 week after the end of 1 year of training (postintervention 2). Measurements will include body composition assessment using anthropometry, dual X-ray absorptiometry and MRI to measure size of different muscle groups. Metabolic profile will include measuring of basal metabolic rate, followed by blood drawn to measure fasting biomarkers similar to hemoglobin A1c, lipid panels, C reactive protein, interleukin-6 and free fatty acids and then intravenous glucose tolerance test to test for insulin sensitivity and glucose effectiveness. Finally, muscle biopsy will be captured to measure protein expression and intracellular signalling; and mitochondrial electron transport chain function. The participants will fill out 3 days dietary record to monitor their energy intake on a weekly basis.
Ethics and dissemination: The study was approved by Institutional Review Board of the McGuire Research Institute (ID # 02189). Dissemination plans will include the Veteran Health Administration and its practitioners, the national SCI/D services office, the general healthcare community and the veteran population, as well as the entire SCI community via submitting quarterly letters or peer-review articles.
Trial registration number: NCT03345576.
Keywords: neurobiology; neuromuscular disease; neurophysiology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials