

Müller cell degeneration and microglial dysfunction in the Alzheimer's retina
- PMID: 36199154
- PMCID: PMC9533552
- DOI: 10.1186/s40478-022-01448-y
Müller cell degeneration and microglial dysfunction in the Alzheimer's retina
Abstract
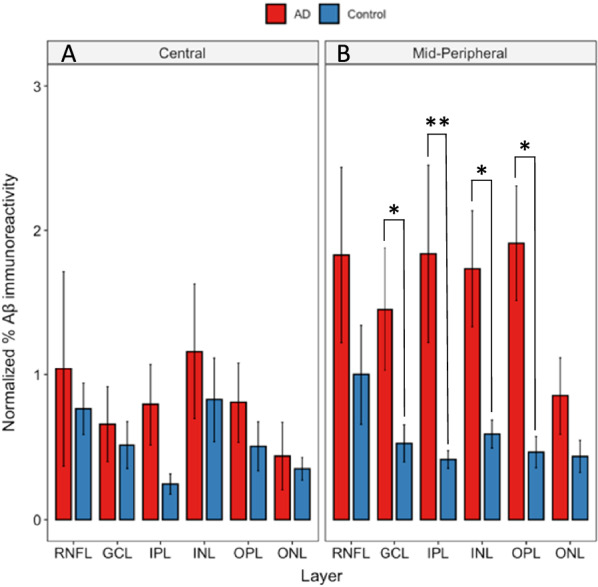
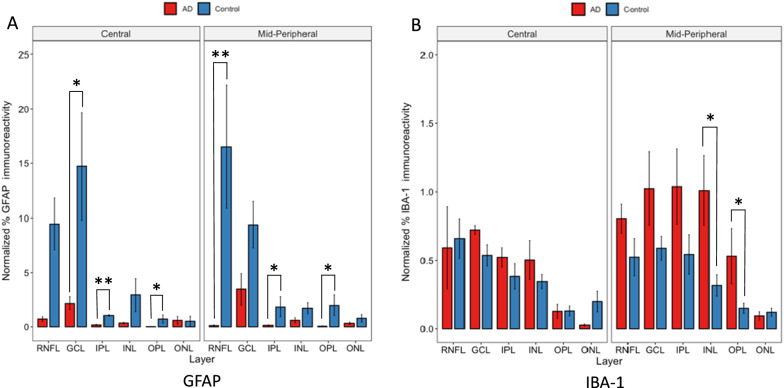
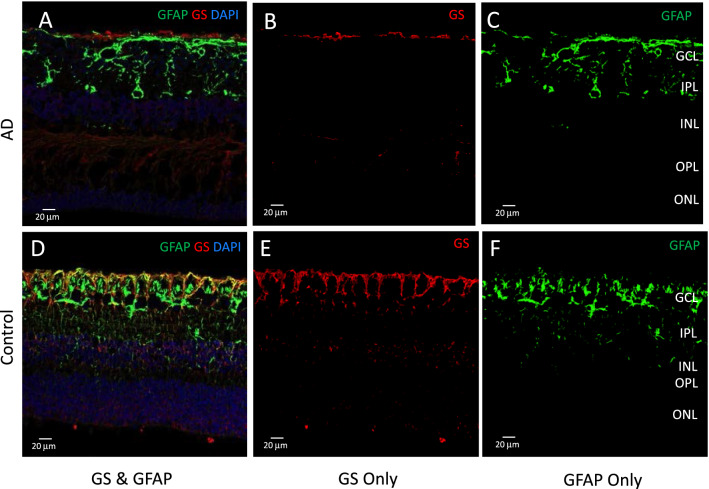
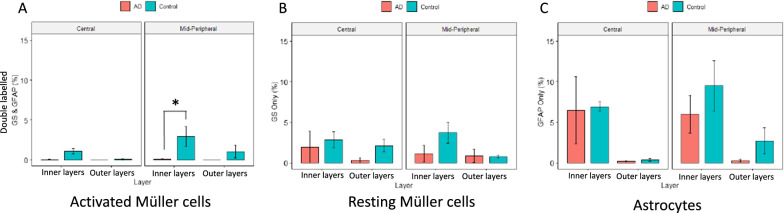
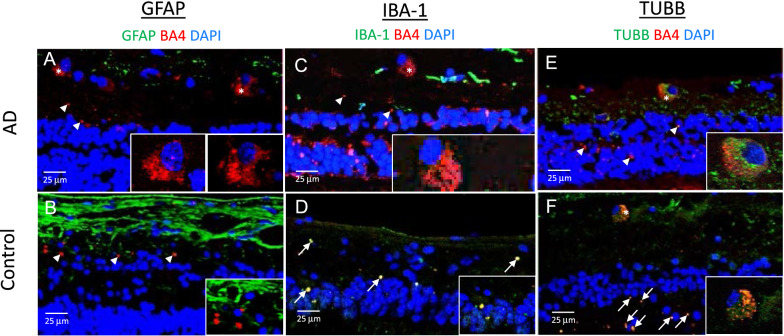
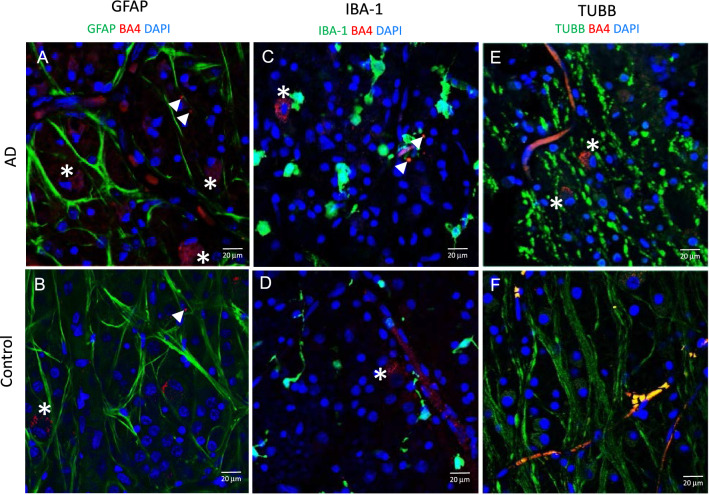
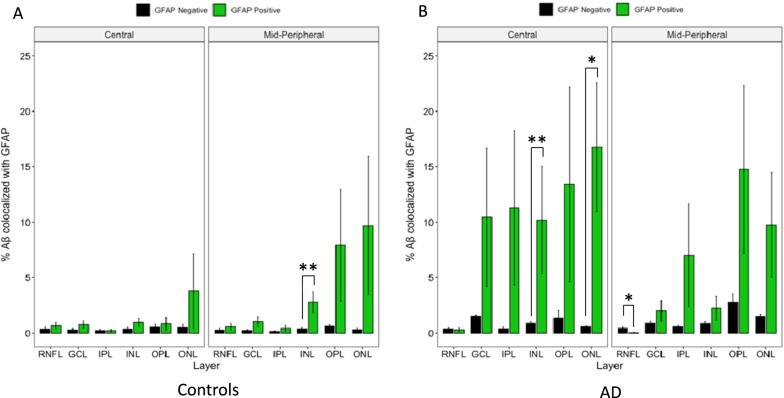
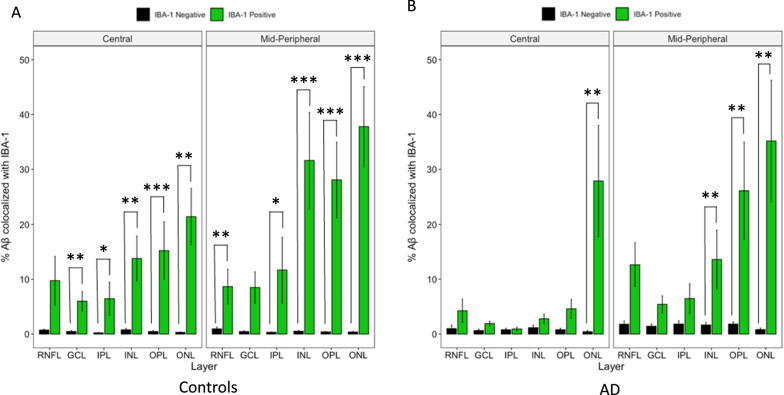
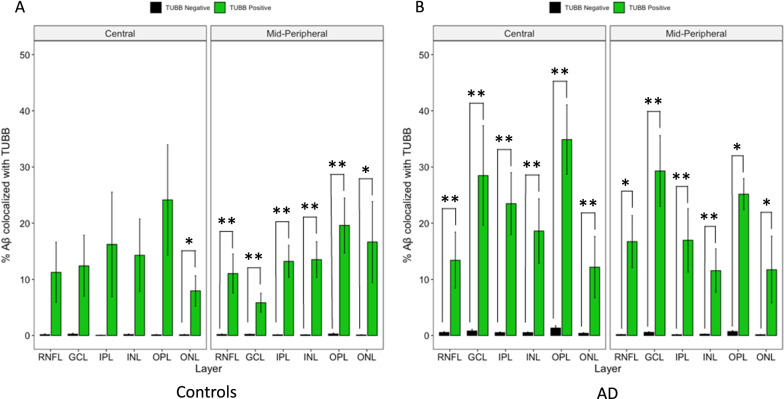
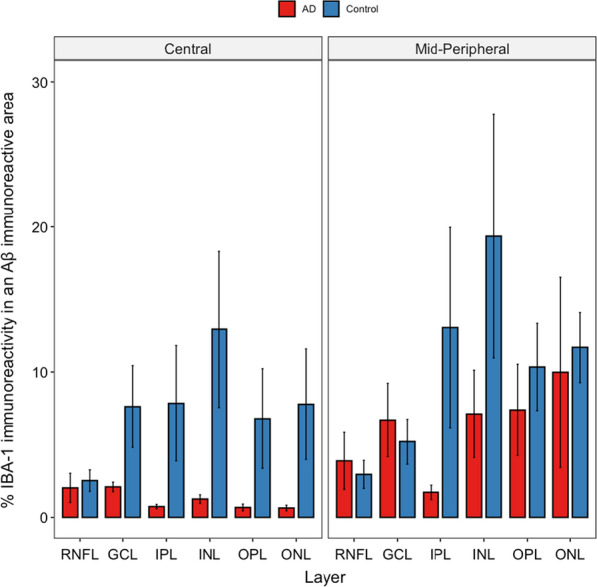
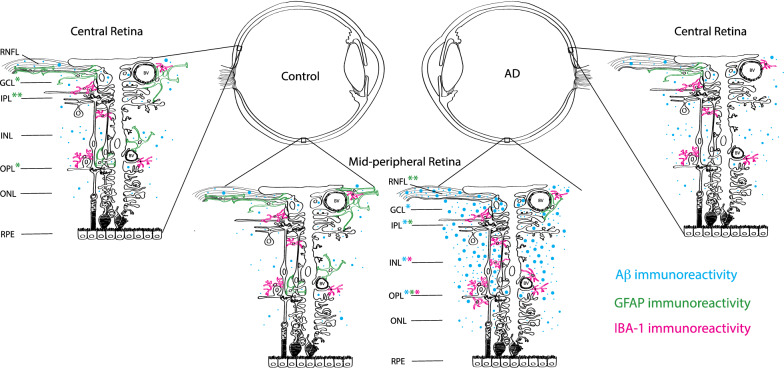
Amyloid beta (Aβ) deposits in the retina of the Alzheimer's disease (AD) eye may provide a useful diagnostic biomarker for AD. This study focused on the relationship of Aβ with macroglia and microglia, as these glial cells are hypothesized to play important roles in homeostasis and clearance of Aβ in the AD retina. Significantly higher Aβ load was found in AD compared to controls, and specifically in the mid-peripheral region. AD retina showed significantly less immunoreactivity against glial fibrillary acidic protein (GFAP) and glutamine synthetase (GS) compared to control eyes. Immunoreactivity against ionized calcium binding adapter molecule-1 (IBA-1), a microglial marker, demonstrated a higher level of microgliosis in AD compared to control retina. Within AD retina, more IBA-1 immunoreactivity was present in the mid-peripheral retina, which contained more Aβ than the central AD retina. GFAP co-localized rarely with Aβ, while IBA-1 co-localized with Aβ in more layers of control than AD donor retina. These results suggest that dysfunction of the Müller and microglial cells may be key features of the AD retina.
Keywords: Alzheimer’s disease; Amyloid-β; Biomarker; Macroglia; Microglia; Retina.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Retinal macroglia changes in a triple transgenic mouse model of Alzheimer's disease.Exp Eye Res. 2014 Oct;127:252-60. doi: 10.1016/j.exer.2014.08.006. Epub 2014 Aug 19. Exp Eye Res. 2014. PMID: 25149907 Free PMC article.
-
Microglial Activation in the Retina of a Triple-Transgenic Alzheimer's Disease Mouse Model (3xTg-AD).Int J Mol Sci. 2020 Jan 27;21(3):816. doi: 10.3390/ijms21030816. Int J Mol Sci. 2020. PMID: 32012676 Free PMC article.
-
Fibrillar Aβ triggers microglial proteome alterations and dysfunction in Alzheimer mouse models.Elife. 2020 Jun 8;9:e54083. doi: 10.7554/eLife.54083. Elife. 2020. PMID: 32510331 Free PMC article.
-
Effects of CX3CR1 and Fractalkine Chemokines in Amyloid Beta Clearance and p-Tau Accumulation in Alzheimer's Disease (AD) Rodent Models: Is Fractalkine a Systemic Biomarker for AD?Curr Alzheimer Res. 2016;13(4):403-12. doi: 10.2174/1567205013666151116125714. Curr Alzheimer Res. 2016. PMID: 26567742 Review.
-
Possible Neuropathology of Sleep Disturbance Linking to Alzheimer's Disease: Astrocytic and Microglial Roles.Front Cell Neurosci. 2022 Jun 9;16:875138. doi: 10.3389/fncel.2022.875138. eCollection 2022. Front Cell Neurosci. 2022. PMID: 35755779 Free PMC article. Review.
Cited by
-
Retinal ganglion cell vulnerability to pathogenic tau in Alzheimer's disease.bioRxiv [Preprint]. 2024 Sep 21:2024.09.17.613293. doi: 10.1101/2024.09.17.613293. bioRxiv. 2024. Update in: Acta Neuropathol Commun. 2025 Feb 15;13(1):31. doi: 10.1186/s40478-025-01935-y. PMID: 39345568 Free PMC article. Updated. Preprint.
-
The Eye as a Diagnostic Tool for Alzheimer's Disease.Life (Basel). 2023 Mar 8;13(3):726. doi: 10.3390/life13030726. Life (Basel). 2023. PMID: 36983883 Free PMC article. Review.
-
3-Dimensional morphological characterization of neuroretinal microglia in Alzheimer's disease via machine learning.Acta Neuropathol Commun. 2024 Dec 24;12(1):202. doi: 10.1186/s40478-024-01898-6. Acta Neuropathol Commun. 2024. PMID: 39719599 Free PMC article.
-
Novel insights into pathomechanisms of retinal neuronal degeneration and reactive gliosis in a murine model of GM1-gangliosidosis.Sci Rep. 2025 Aug 13;15(1):29674. doi: 10.1038/s41598-025-15639-9. Sci Rep. 2025. PMID: 40804287 Free PMC article.
-
Chlamydia pneumoniae in Alzheimer's disease pathology.Front Neurosci. 2024 May 6;18:1393293. doi: 10.3389/fnins.2024.1393293. eCollection 2024. Front Neurosci. 2024. PMID: 38770241 Free PMC article. Review.
References
-
- Alzheimer’s A (2015) 2015 Alzheimer's disease facts and figures. Alzheimer's & dementia. J Alzheimer's Association, 11:332 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
