

Incidence and Predictors of Recurrence and Mortality Following First Venous Thromboembolism Among the Saudi Population: Single-Center Cohort Study
- PMID: 36199587
- PMCID: PMC9527814
- DOI: 10.2147/IJGM.S359893
Incidence and Predictors of Recurrence and Mortality Following First Venous Thromboembolism Among the Saudi Population: Single-Center Cohort Study
Abstract
Background: Little is written about recurrence and mortality rates after a first episode of venous thromboembolism (VTE) among Saudi population.
Aim: Determine incidence rates and assess predictors of recurrence and mortality following the first VTE event.
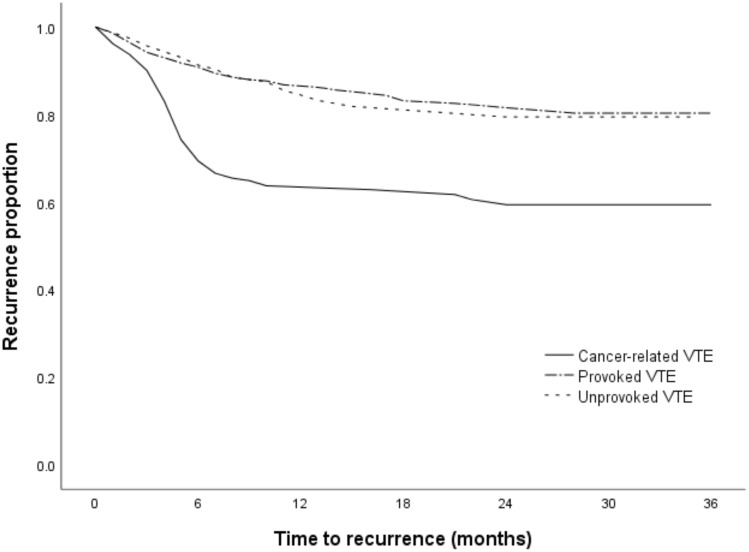
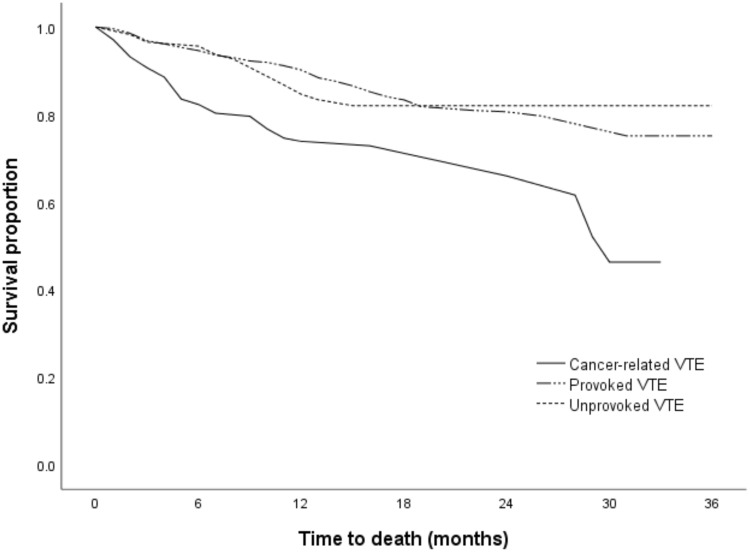
Patients and methods: A total of 1124 patients aged ≥18 years with symptomatic VTE confirmed by imaging tests were evaluated. The incidence of VTE recurrence and mortality were assessed. The association between patient characteristics, and VTE recurrence and mortality was explored by estimating the hazard ratio (HR) and 95% confidence interval (CI). The difference between cancer-related, provoked and unprovoked VTE in terms of recurrence and mortality was explored using Kaplan-Meier curves.
Results: The annual incidence rate of the first VTE was 1.7 per 1000 patients. Of 1124 patients with first VTE, 214 (19%) developed recurrent VTE, and 192 (17%) died with overall incidence rates of 15.8 per 100 person-years (95% CI, 13.8-18.0) and 10.0 per 100 person-years (95% CI, 8.7-11.5). Intensive care unit (ICU) admission (HR, 2.15; 95% CI, 1.67-3.10), presence of active cancer (HR, 2.97; 95% CI, 1.87-3.95), immobilization (HR, 2.52; 95% CI, 1.79-3.67), infection (HR, 2.32; 95% CI, 1.94-3.45), and pulmonary embolism ± deep venous thrombosis (HR, 2.22; 95% CI, 1.56-3.16) were found to be independent predictors of recurrent VTE. Recurrence carries a high hazard of mortality (HR, 5.21; 95% CI, 3.61-7.51). The estimated median time to VTE recurrence was lower in cancer-related VTE (18.7 months) compared with provoked (29.0 months) and unprovoked VTE (28.4 months). The estimated survival median time was lower in cancer-related VTE (21.8 months) compared with provoked (30.5 months) and unprovoked VTE (29.8 months).
Conclusion: Immobilization and presence of active cancer, infection, and PE ± DVT were significant predictors of recurrent VTE. Patients who developed recurrent VTE had a 5.2-fold higher hazard of mortality compared with patients with no VTE recurrence.
Keywords: active cancer; incidence; mortality; predictors; recurrent; venous thromboembolism.
© 2022 AlEidan et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Risk of recurrent venous thromboembolism in patients with HIV infection: A nationwide cohort study.PLoS Med. 2020 May 14;17(5):e1003101. doi: 10.1371/journal.pmed.1003101. eCollection 2020 May. PLoS Med. 2020. PMID: 32407386 Free PMC article.
-
The risk of recurrent venous thromboembolism in patients with unprovoked symptomatic deep vein thrombosis and asymptomatic pulmonary embolism.Thromb Haemost. 2006 Mar;95(3):562-6. doi: 10.1160/TH05-10-0677. Thromb Haemost. 2006. PMID: 16525588
-
Incidence and Risk Factors of Recurrent Venous Thromboembolism after Pulmonary Embolism.Tuberc Respir Dis (Seoul). 2019 Oct;82(4):341-347. doi: 10.4046/trd.2019.0019. Epub 2019 May 31. Tuberc Respir Dis (Seoul). 2019. PMID: 31172708 Free PMC article.
-
Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis.BMJ. 2019 Jul 24;366:l4363. doi: 10.1136/bmj.l4363. BMJ. 2019. PMID: 31340984 Free PMC article.
-
Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism.Ann Intern Med. 2010 Oct 19;153(8):523-31. doi: 10.7326/0003-4819-153-8-201010190-00009. Ann Intern Med. 2010. PMID: 20956709 Review.
Cited by
-
Diagnostic approach and use of CTPA in patients with suspected pulmonary embolism in an emergency department in Saudi Arabia.Blood Res. 2023 Mar 31;58(1):51-60. doi: 10.5045/br.2023.2023007. Epub 2023 Mar 16. Blood Res. 2023. PMID: 36922446 Free PMC article.
-
Clinical Features and Predictors of Mortality in Patients With Acute Pulmonary Embolism: A Retrospective Study From Southern Saudi Arabia.Cureus. 2024 Mar 6;16(3):e55623. doi: 10.7759/cureus.55623. eCollection 2024 Mar. Cureus. 2024. PMID: 38586707 Free PMC article.
-
Incidence Rate of Cardiovascular Events in Rheumatoid Arthritis: An Observational Cohort Study in Saudi Arabia.J Multidiscip Healthc. 2024 Jul 12;17:3357-3370. doi: 10.2147/JMDH.S459555. eCollection 2024. J Multidiscip Healthc. 2024. PMID: 39045492 Free PMC article.
-
The Incidence, Risk Factors and Characteristics of Late (>2 Years) Recurrence of Deep Venous Thrombosis.Clin Appl Thromb Hemost. 2025 Jan-Dec;31:10760296251332937. doi: 10.1177/10760296251332937. Epub 2025 Apr 13. Clin Appl Thromb Hemost. 2025. PMID: 40221979 Free PMC article.
-
Is CT pulmonary angiography overutilized in the evaluation of patients with suspected pulmonary embolism? A retrospective study.Can J Respir Ther. 2025 Jan 13;61:127660. doi: 10.29390/001c.127660. eCollection 2025. Can J Respir Ther. 2025. PMID: 39822304 Free PMC article.
References
-
- El Margoushy NM, Al-Suwat RW, Al-Otaibi WA, Mougrabi MM. Incidence of pulmonary embolism in CCU at King Faisal hospital, Taif, Saudi Arabia. Egypt J Hospital Med. 2017;68(1):865–877. doi:10.12816/0038185 - DOI
LinkOut - more resources
Full Text Sources
