

Low-dose norepinephrine in combination with hypotensive resuscitation may prolong the golden window for uncontrolled hemorrhagic shock in rats
- PMID: 36200050
- PMCID: PMC9527312
- DOI: 10.3389/fphys.2022.1004714
Low-dose norepinephrine in combination with hypotensive resuscitation may prolong the golden window for uncontrolled hemorrhagic shock in rats
Abstract
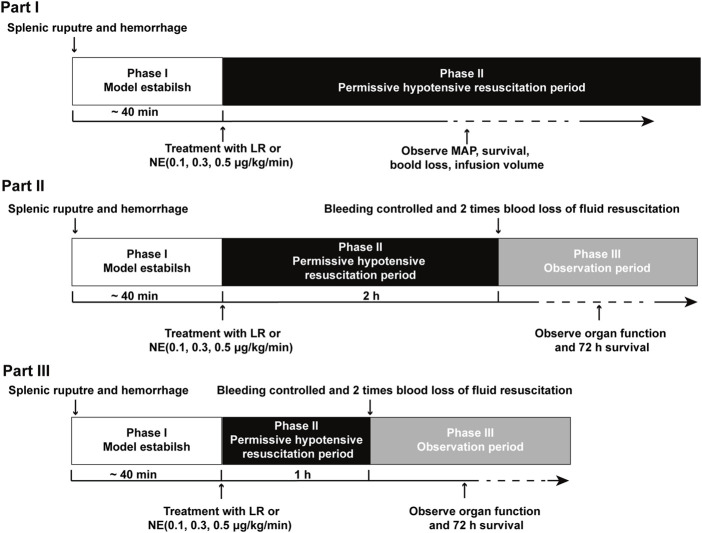
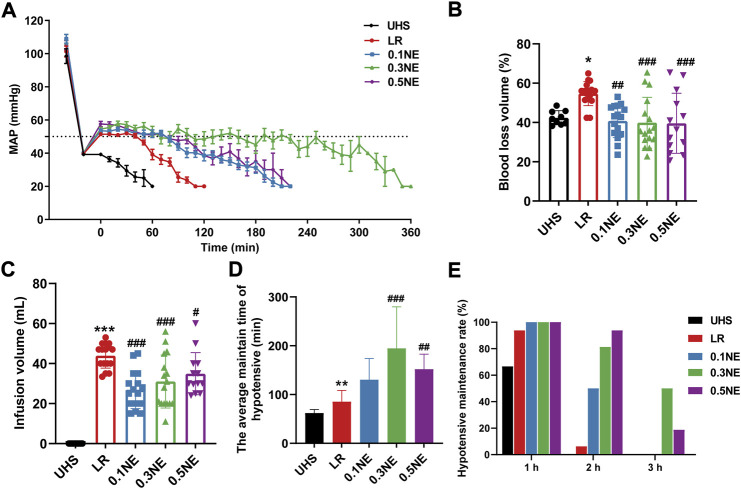
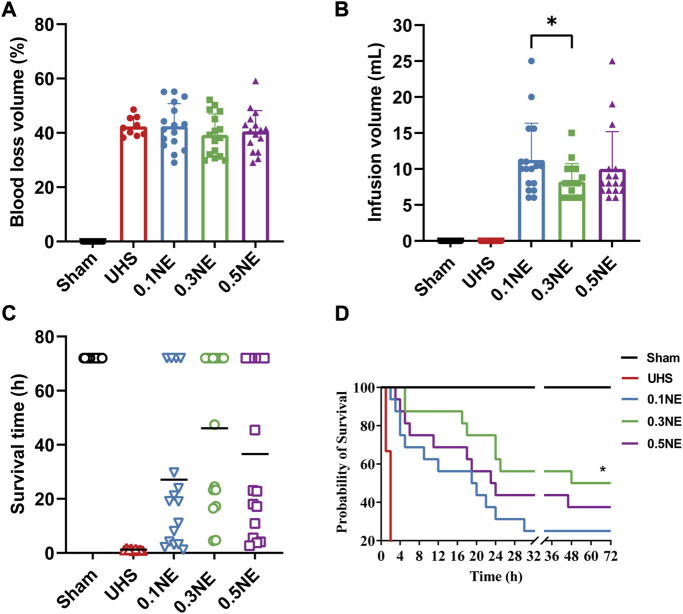
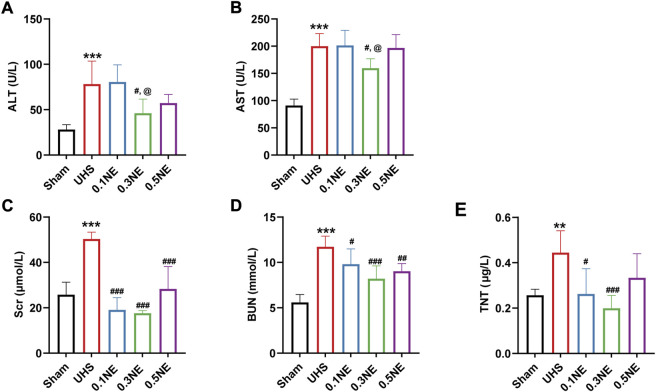
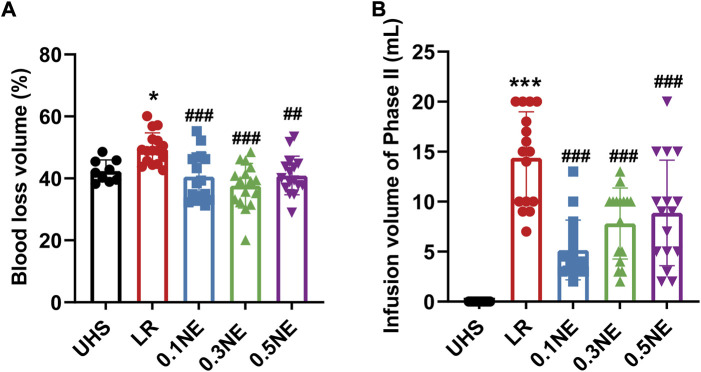
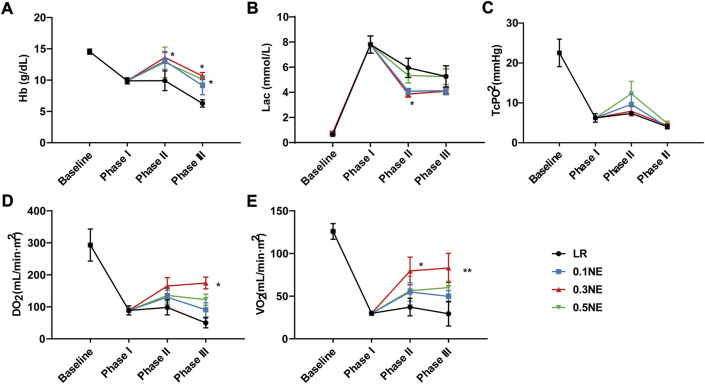
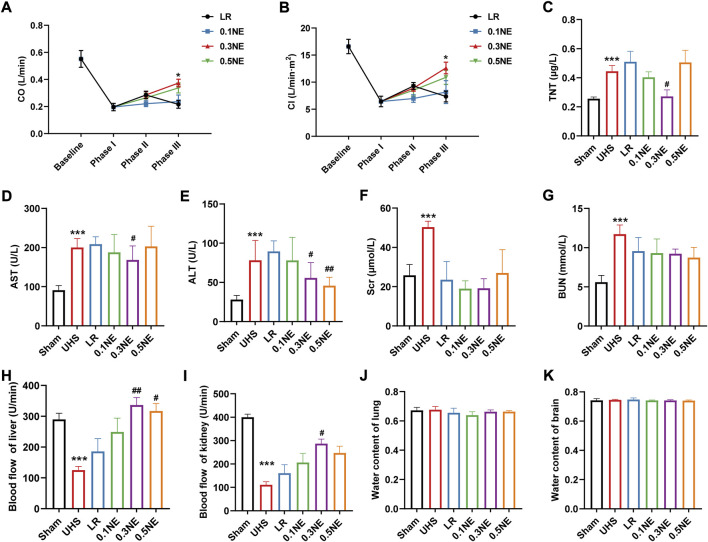
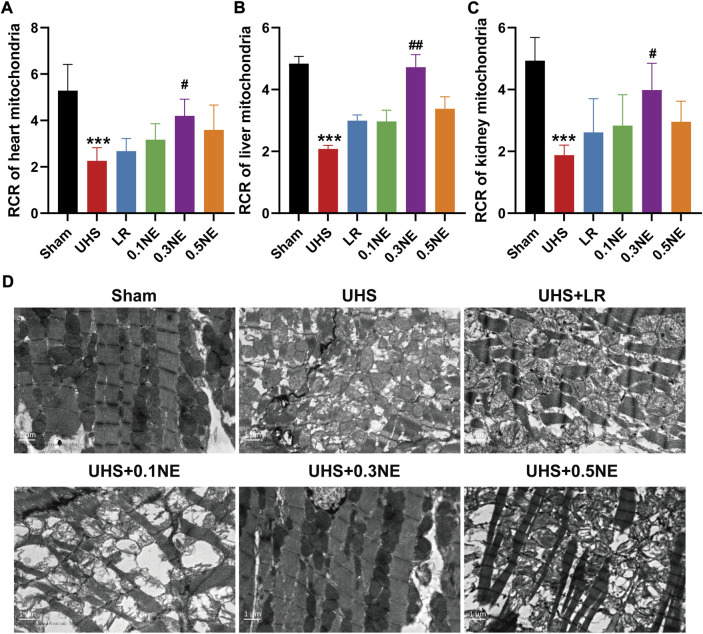
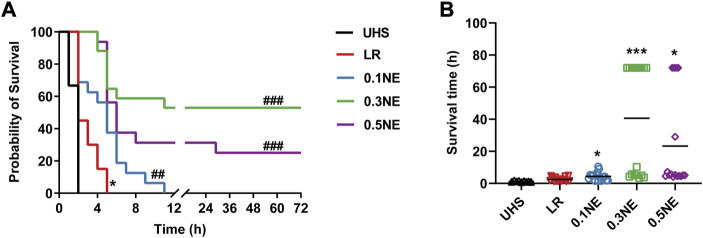
Hypotension resuscitation is an important principle for the treatment after trauma. Current hypotensive resuscitation strategies cannot obtain an ideal outcome for remote regions. With the uncontrolled hemorrhagic shock (UHS) model in rats, the effects of norepinephrine (NE) on the tolerance time of hypotensive resuscitation, blood loss, vital organ functions, and animal survival were observed. Before bleeding was controlled, only the LR infusion could effectively maintain the MAP to 50-60 mmHg for 1 h, while the MAP gradually decreased with prolonging time, even with increasing infusion volume. Low-dose NE during hypotensive resuscitation prolonged the hypotensive tolerance time to 2-3 h, and the effect of 0.3 μg/kg/min NE was the best. Further studies showed that 0.3 μg/kg/min NE during hypotensive resuscitation significantly lightened the damage of organ function induced by UHS via protecting mitochondrial function, while the LR infusion did not. At the same time, NE administration improved Hb content, DO2, and VO2, and restored liver and kidney blood flow. The survival results showed that low-dose NE administration increased the survival rate and prolonged the survival time. Together, low-dose NE during hypotensive resuscitation was suitable for the early treatment of UHS, which can strive for the golden window of emergency treatment for serious trauma patients by reducing blood loss and protecting vital organ functions.
Keywords: golden treatment time; hypotension resuscitation; norepinephrine; organ function; uncontrolled hemorrhagic shock.
Copyright © 2022 Zhou, Li, Xiang, Wu, Zhu, Peng, Liu and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Cardinale M., Cungi P. J., Esnault P., Nguyen C., Cotte J., Montcriol A., et al. (2020). Impact of high-dose norepinephrine during intra-hospital damage control resuscitation of traumatic haemorrhagic shock: a propensity-score analysis. Injury 51, 1164–1171. 10.1016/j.injury.2019.11.037 - DOI - PubMed
-
- Das J. M., Anosike K., Waseem M. (2022). “Permissive hypotension,” in StatPearls (Treasure Island (FL): StatPearls Publishing LLC.) StatPearls Publishing Copyright © 2022. - PubMed
LinkOut - more resources
Full Text Sources