

Isolated popliteal artery lesion due to giant cell vasculitis post COVID-19 mRNA vaccine and COVID-19 asymptomatic infection
- PMID: 36200437
- PMCID: PMC9535462
- DOI: 10.1177/17085381221126234
Isolated popliteal artery lesion due to giant cell vasculitis post COVID-19 mRNA vaccine and COVID-19 asymptomatic infection
Abstract
Objective: Giant cell arteritis (GCA) is a rare granulomatous vasculitis, affecting medium and large vessels, usually in old patients. The incidence of GCA has been higher during current COVID-19 pandemia and COVID-19 is recognized for its immune dysregulation. Lower limbs involvement is uncommon but can be limb threatening, resulting in limb loss.
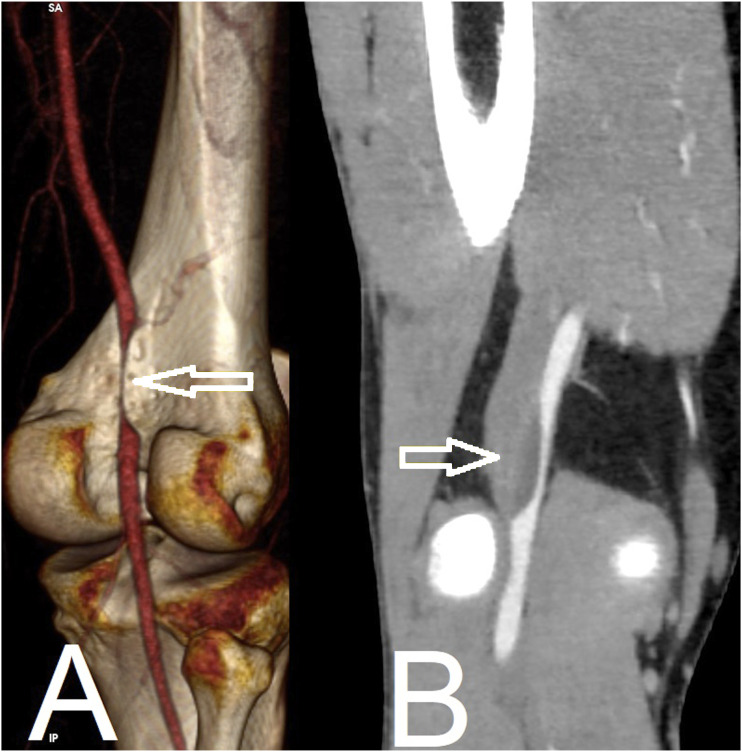
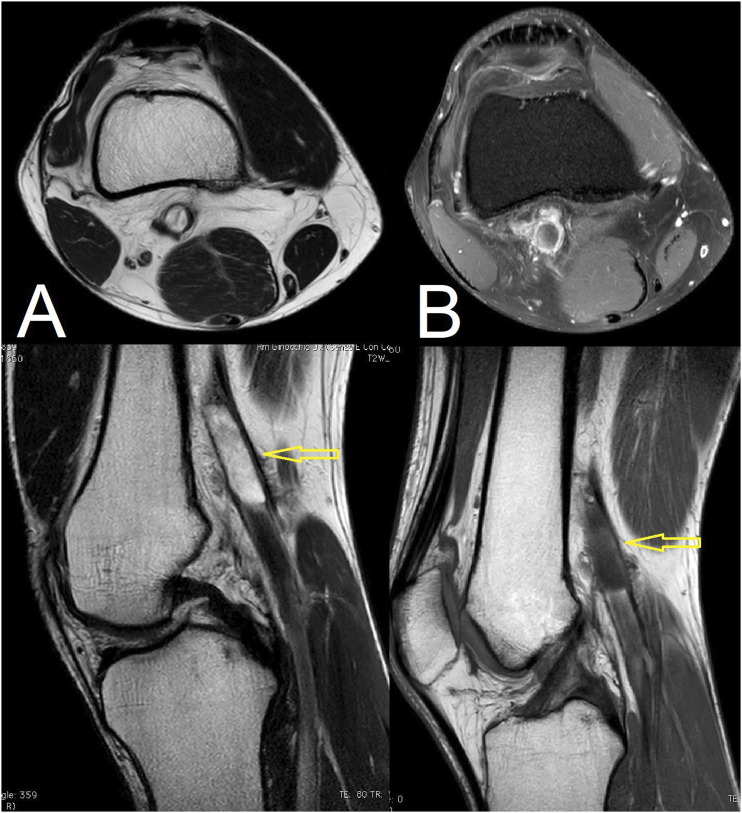
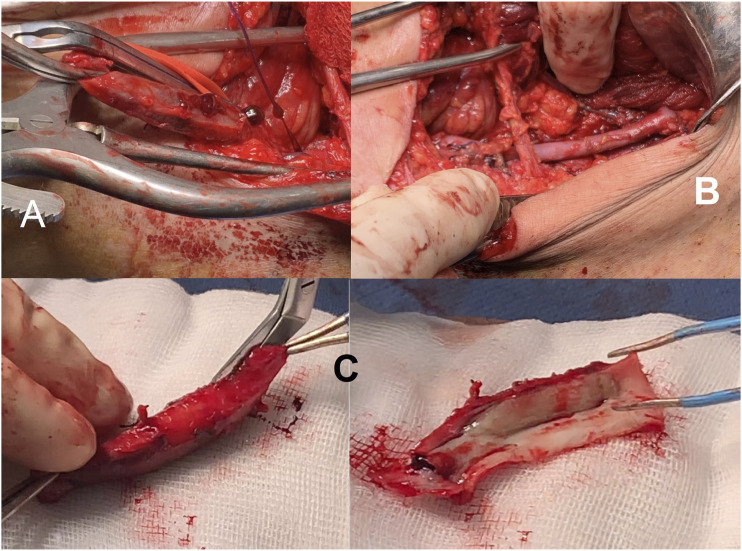
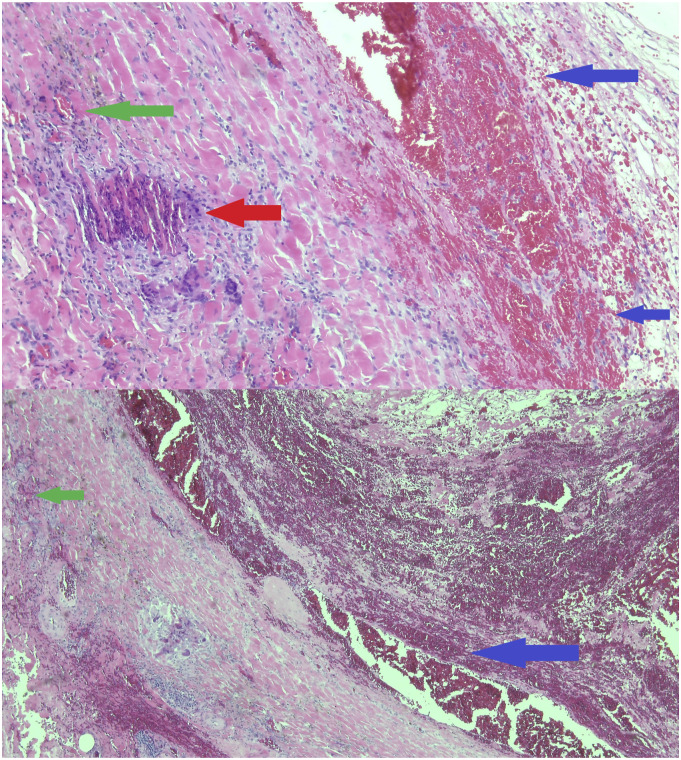
Method: A 43-year-old man presented with a sudden pain in his right calf and foot associated with pallor and hypothermia, and there was objective evidence of ischemia. Symptoms began few days after he received the first dose of a COVID-19 mRNA vaccine and COVID-19 asymptomatic infection 20 days after vaccination. He had no history of any signs of claudication pre-COVID or limb trauma and was very fit.Enhanced computed tomography and magnetic resonance imaging (MRI)suggest diagnosis of popliteal artery cystic adventitial disease. We resected the affected popliteal artery with interposition using a right great saphenous vein graft, through a posterior approach. On the fourth postoperative day, he was discharged.Histopathological examination revealed patchy intramural inflammatory infiltrates composed of lymphocytes and rare multinucleated giant cells at the internal lamina and adventitia consistent with a diagnosis of GCA.
Conclusion and result: Our case represents the first reported case of isolated popliteal GCA following vaccination with a COVID-19 mRNA vaccine and COVID-19 infection. We propose that the upregulated immune response to the vaccine acted as a trigger for GCA in this patient with predisposing risk factors and recurrent and repetitive microtrauma in popliteal fossa (the patient is a professional runner). Our case suggests the need for further studies about real world incidence of GCA associated vaccination and COVID-19 infection. Currently, data is limited regarding this relationship. We continue to encourage COVID-19 vaccination, even in elderly patients because the benefits of vaccination far outweigh any theoretical risk of immune dysregulation following administration.
Keywords: covid-19; giant cell arteritis; immunization; vaccine.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Tatò F, Hoffmann U. Giant cell arteritis: a systemic vascular disease. Vasc Med 2008; 13: 127–140. - PubMed
-
- Danesh-Meyer H, Savino PJ, Gamble GG. Poor prognosis of visual outcome after visual loss from giant cell0020arteritis. Ophthalmology 2005; 112: 1098–1103. - PubMed
-
- Kermani TA, Matteson EL, Hunder GG, et al.Symptomatic lower extremity vasculitis in giant cell arteritis: a case series. J Rheumatol 2009; 36: 2277–2283. - PubMed
-
- Terrades-Garcia N, Cid MC. Pathogenesis of giant-cell arteritis: how targeted therapies are influencing our understanding of the mechanisms involved. Rheumatology 2018; 57: 51–62. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
