

Machine learning evaluation of LV outflow obstruction in hypertrophic cardiomyopathy using three-chamber cardiovascular magnetic resonance
- PMID: 36201099
- PMCID: PMC9708771
- DOI: 10.1007/s10554-022-02724-7
Machine learning evaluation of LV outflow obstruction in hypertrophic cardiomyopathy using three-chamber cardiovascular magnetic resonance
Abstract
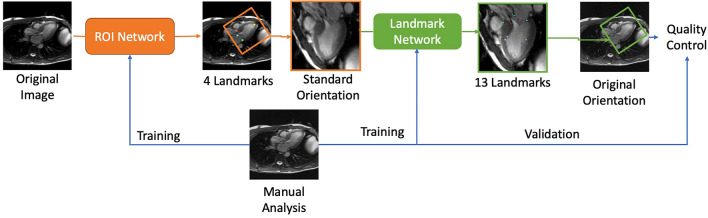
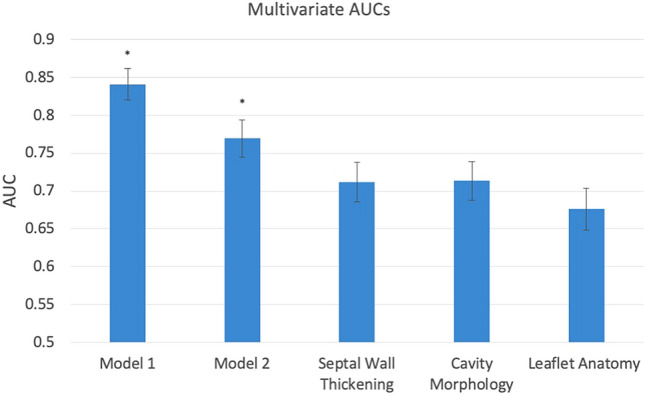
Left ventricular outflow tract obstruction (LVOTO) is common in hypertrophic cardiomyopathy (HCM), but relationships between anatomical metrics and obstruction are poorly understood. We aimed to develop machine learning methods to evaluate LVOTO in HCM patients and quantify relationships between anatomical metrics and obstruction. This retrospective analysis of 1905 participants of the HCM Registry quantified 11 anatomical metrics derived from 14 landmarks automatically detected on the three-chamber long axis cine CMR images. Linear and logistic regression was used to quantify strengths of relationships with the presence of LVOTO (defined by resting Doppler pressure drop of > 30 mmHg), using the area under the receiver operating characteristic (AUC). Intraclass correlation coefficients between the network predictions and three independent observers showed similar agreement to that between observers. The distance from anterior mitral valve leaflet tip to basal septum (AML-BS) was most highly correlated with Doppler pressure drop (R2 = 0.19, p < 10-5). Multivariate stepwise regression found the best predictive model included AML-BS, AML length to aortic valve diameter ratio, AML length to LV width ratio, and midventricular septal thickness metrics (AUC 0.84). Excluding AML-BS, metrics grouped according to septal hypertrophy, LV geometry, and AML anatomy each had similar associations with LVOTO (AUC 0.71, 0.71, 0.68 respectively, p = ns), significantly less than their combination (AUC 0.77, p < 0.05 for each). Anatomical metrics derived from a standard three-chamber CMR cine acquisition can be used to highlight risk of LVOTO, and suggest further investigation if necessary. A combination of geometric factors is required to provide the best risk prediction.
Keywords: Atlas shape analysis; Hypertrophic cardiomyopathy; LV outflow tract obstruction.
© 2022. The Author(s).
Conflict of interest statement
Dr. Neubauer has been a consultant for Pfizer and Cytokinetics; and has received research grants from Boehringer Ingelheim. Dr. Kwong has received research support from Siemens Healthineers, Bayer AG, and MyoKardia. Dr. Schulz-Menger has been a consultant for Bayer; and has received research grants from Bayer, Siemens Healthineers, and Circle Cardiovascular Imaging. Dr Weintraub has been a consultant for Amarin, Janssen, AstraZeneca, and SC Pharma, and has received research grants from Amarin. Dr. Kramer has been a consultant for Cytokinetics; and has received research grants from Biotelemetry and MyoKardia. Other authors have nothing to disclose.
Figures


Comment in
-
Editor's choice to the December 2022 issue : Machine learning evaluation of LV outflow obstruction in hypertrophic cardiomyopathy using threechamber cardiovascular magnetic resonance.Int J Cardiovasc Imaging. 2022 Dec;38(12):2511-2512. doi: 10.1007/s10554-022-02758-x. Int J Cardiovasc Imaging. 2022. PMID: 36396751 No abstract available.
Similar articles
-
Contribution of mitral valve leaflet length and septal wall thickness to outflow tract obstruction in patients with hypertrophic cardiomyopathy.Int J Cardiovasc Imaging. 2017 Aug;33(8):1201-1211. doi: 10.1007/s10554-017-1103-5. Epub 2017 Apr 8. Int J Cardiovasc Imaging. 2017. PMID: 28391581
-
Evaluation of potential links between phenotypic features and genetic variants in left ventricular outflow tract obstruction in hypertrophic cardiomyopathy using cardiovascular magnetic resonance imaging.Int J Cardiovasc Imaging. 2024 Nov;40(11):2417-2428. doi: 10.1007/s10554-024-03250-4. Epub 2024 Sep 30. Int J Cardiovasc Imaging. 2024. PMID: 39347935
-
Long mitral valve leaflets determine left ventricular outflow tract obstruction during exercise in hypertrophic cardiomyopathy.Int J Cardiol. 2016 Jun 1;212:47-53. doi: 10.1016/j.ijcard.2016.03.041. Epub 2016 Mar 16. Int J Cardiol. 2016. PMID: 27031819
-
The Role of the Submitral Apparatus in Hypertrophic Obstructive Cardiomyopathy.J Am Soc Echocardiogr. 2023 Feb;36(2):133-145. doi: 10.1016/j.echo.2022.09.018. Epub 2022 Sep 30. J Am Soc Echocardiogr. 2023. PMID: 36191671 Review.
-
The 50-year history, controversy, and clinical implications of left ventricular outflow tract obstruction in hypertrophic cardiomyopathy from idiopathic hypertrophic subaortic stenosis to hypertrophic cardiomyopathy: from idiopathic hypertrophic subaortic stenosis to hypertrophic cardiomyopathy.J Am Coll Cardiol. 2009 Jul 14;54(3):191-200. doi: 10.1016/j.jacc.2008.11.069. J Am Coll Cardiol. 2009. PMID: 19589431 Review.
Cited by
-
Left ventricular anatomy in obstructive hypertrophic cardiomyopathy: beyond basal septal hypertrophy.Eur Heart J Cardiovasc Imaging. 2023 May 31;24(6):807-818. doi: 10.1093/ehjci/jeac233. Eur Heart J Cardiovasc Imaging. 2023. PMID: 36441173 Free PMC article.
-
Editor's choice to the December 2022 issue : Machine learning evaluation of LV outflow obstruction in hypertrophic cardiomyopathy using threechamber cardiovascular magnetic resonance.Int J Cardiovasc Imaging. 2022 Dec;38(12):2511-2512. doi: 10.1007/s10554-022-02758-x. Int J Cardiovasc Imaging. 2022. PMID: 36396751 No abstract available.
-
Exploring the Current Status of Risk Stratification in Hypertrophic Cardiomyopathy: From Risk Models to Promising Techniques.J Cardiovasc Dev Dis. 2025 Mar 14;12(3):101. doi: 10.3390/jcdd12030101. J Cardiovasc Dev Dis. 2025. PMID: 40137099 Free PMC article. Review.
-
Spatial relationship between mitral valve and ventricular septum assessed by resting echocardiography to diagnose left ventricular outflow tract obstruction in hypertrophic cardiomyopathy.Eur Heart J Cardiovasc Imaging. 2023 May 31;24(6):710-718. doi: 10.1093/ehjci/jead036. Eur Heart J Cardiovasc Imaging. 2023. PMID: 36841935 Free PMC article.
References
-
- Hypertropic cardiomyopathy | British Heart Foundation. https://www.bhf.org.uk/informationsupport/conditions/cardiomyopathy/hype.... Accessed 30 Nov 2021
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
