

Pooled Analysis of Meningioma Risk Following Treatment for Childhood Cancer
- PMID: 36201196
- PMCID: PMC9539736
- DOI: 10.1001/jamaoncol.2022.4425
Pooled Analysis of Meningioma Risk Following Treatment for Childhood Cancer
Erratum in
-
Change of Article Status to Open Access.JAMA Oncol. 2022 Nov 10;8(12):1856. doi: 10.1001/jamaoncol.2022.6336. Online ahead of print. JAMA Oncol. 2022. PMID: 36355366 Free PMC article. No abstract available.
Abstract
Importance: Meningioma is the most common subsequent neoplasm following cranial irradiation among survivors of childhood cancer, but there are still uncertainties regarding the magnitude of the radiation dose-response association, potential modifiers of radiation risks, and the role of chemotherapy.
Objective: To evaluate meningioma risk in survivors of childhood cancer following radiotherapy and chemotherapy and identify possible modifying factors of radiation-associated risk.
Design, setting, and participants: This international case-control study pooled data from 4 nested case-control studies of survivors of childhood cancer diagnosed between 1942 and 2000, followed through 2016. Cases were defined as participants diagnosed with a subsequent meningioma. Controls were matched to cases based on sex, age at first cancer diagnosis, and duration of follow-up. Data were analyzed from July 2019 to June 2022.
Exposures: Radiation dose (Gy) to the meningioma site and cumulative chemotherapy doses, including intrathecal and systemic methotrexate doses.
Main outcomes and measures: The main outcome was subsequent meningioma, assessed using odds ratios (ORs) and excess odds ratios per gray (EOR/Gy).
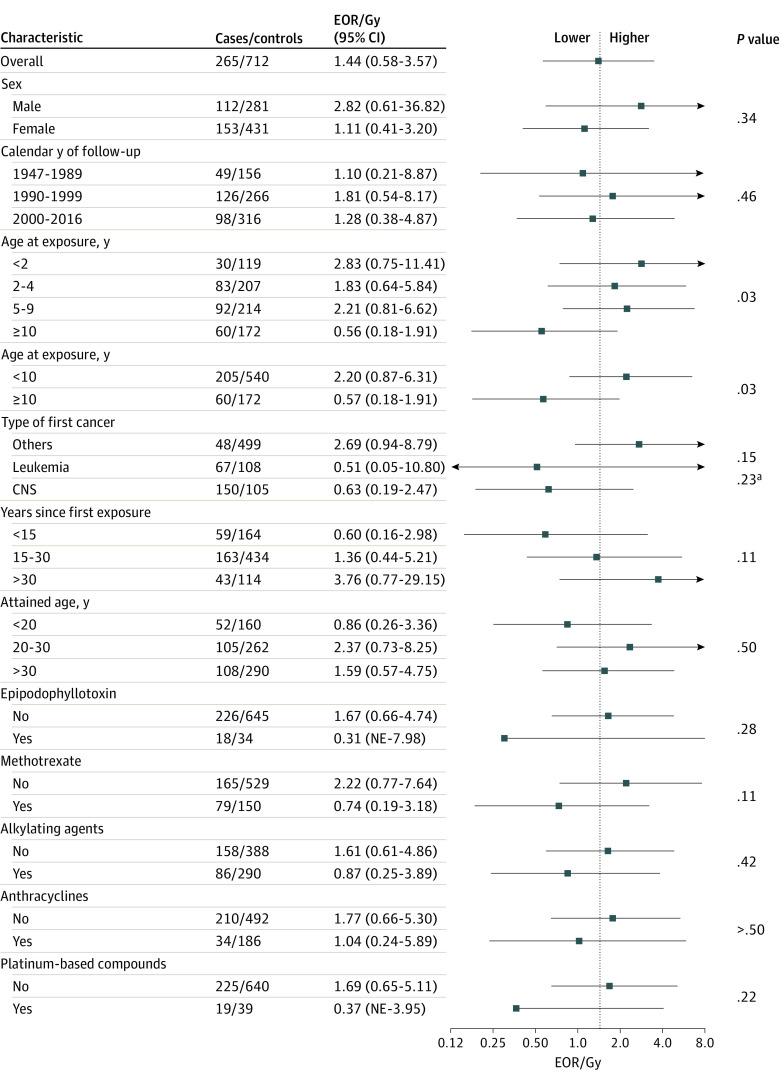
Results: The analysis included 273 survivors of childhood cancer who developed meningioma (cases) and 738 survivors who did not (controls), with a total of 1011 individuals (median [IQR] age at first cancer diagnosis 5.0 [3.0-9.2] years; 599 [59.2%] female). Median (IQR) time since first cancer was 21.5 (15.0-27.0) years. Increasing radiation dose was associated with increased risk of meningioma (EOR/Gy, 1.44; 95% CI, 0.62-3.61), and there was no evidence of departure from linearity (P = .90). Compared with survivors who were not exposed to radiation therapy, those who received doses of 24 Gy or more had more than 30-fold higher odds of meningioma (OR, 33.66; 95% CI, 14.10-80.31). The radiation dose-response association was significantly lower among patients treated at age 10 years or older compared with those treated before age 10 years (EOR/Gy, 0.57; 95% CI, 0.18-1.91 vs 2.20; 95% CI, 0.87-6.31; P for heterogeneity = .03). Risk associated with radiation remained significantly elevated 30 years after exposure (EOR/Gy, 3.76; 95% CI, 0.77-29.15). We found an increased risk of meningioma among children who had received methotrexate (OR, 3.43; 95% CI, 1.56-7.57), but no evidence of a dose-response association or interaction with radiation dose.
Conclusions and relevance: These findings suggest that the meninges are highly radiosensitive, especially for children treated before age 10 years. These results support the reduction in whole-brain irradiation over recent decades and the prioritization of approaches that limit radiation exposure in healthy tissue for children. The persistence of elevated risks of meningiomas for 30 years after cranial radiotherapy could help inform surveillance guidelines.
Conflict of interest statement
Figures

References
-
- Bowers DC, Verbruggen LC, Kremer LCM, et al. Surveillance for subsequent neoplasms of the CNS for childhood, adolescent, and young adult cancer survivors: a systematic review and recommendations from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2021;22(5):e196-e206. doi: 10.1016/S1470-2045(20)30688-4 - DOI - PubMed
