

Respiratory Virus Surveillance Among Children with Acute Respiratory Illnesses - New Vaccine Surveillance Network, United States, 2016-2021
- PMID: 36201373
- PMCID: PMC9541034
- DOI: 10.15585/mmwr.mm7140a1
Respiratory Virus Surveillance Among Children with Acute Respiratory Illnesses - New Vaccine Surveillance Network, United States, 2016-2021
Abstract
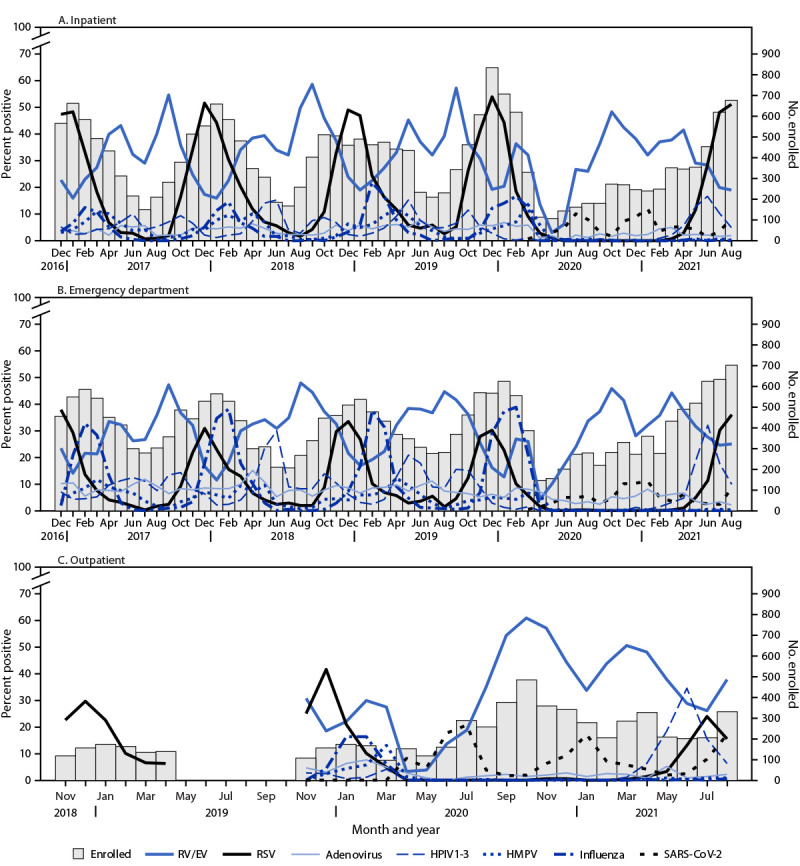
The New Vaccine Surveillance Network (NVSN) is a prospective, active, population-based surveillance platform that enrolls children with acute respiratory illnesses (ARIs) at seven pediatric medical centers. ARIs are caused by respiratory viruses including influenza virus, respiratory syncytial virus (RSV), human metapneumovirus (HMPV), human parainfluenza viruses (HPIVs), and most recently SARS-CoV-2 (the virus that causes COVID-19), which result in morbidity among infants and young children (1-6). NVSN estimates the incidence of pathogen-specific pediatric ARIs and collects clinical data (e.g., underlying medical conditions and vaccination status) to assess risk factors for severe disease and calculate influenza and COVID-19 vaccine effectiveness. Current NVSN inpatient (i.e., hospital) surveillance began in 2015, expanded to emergency departments (EDs) in 2016, and to outpatient clinics in 2018. This report describes demographic characteristics of enrolled children who received care in these settings, and yearly circulation of influenza, RSV, HMPV, HPIV1-3, adenovirus, human rhinovirus and enterovirus (RV/EV),* and SARS-CoV-2 during December 2016-August 2021. Among 90,085 eligible infants, children, and adolescents (children) aged <18 years† with ARI, 51,441 (57%) were enrolled, nearly 75% of whom were aged <5 years; 43% were hospitalized. Infants aged <1 year accounted for the largest proportion (38%) of those hospitalized. The most common pathogens detected were RV/EV and RSV. Before the emergence of SARS-CoV-2, detected respiratory viruses followed previously described seasonal trends, with annual peaks of influenza and RSV in late fall and winter (7,8). After the emergence of SARS-CoV-2 and implementation of associated pandemic nonpharmaceutical interventions and community mitigation measures, many respiratory viruses circulated at lower-than-expected levels during April 2020-May 2021. Beginning in summer 2021, NVSN detected higher than anticipated enrollment of hospitalized children as well as atypical interseasonal circulation of RSV. Further analyses of NVSN data and continued surveillance are vital in highlighting risk factors for severe disease and health disparities, measuring the effectiveness of vaccines and monoclonal antibody-based prophylactics, and guiding policies to protect young children from pathogens such as SARS-CoV-2, influenza, and RSV.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Janet A. Englund reports support from AstraZeneca, GSK (GlaxoSmithKline), and Pfizer, Inc., and consulting fees from Sanofi Pasteur, Meissa Vaccines, and AstraZeneca. Natasha B. Halasa reports grant support from Sanofi Pasteur and Quidel and an education grant from Genetech. Christopher J. Harrison reports institutional support from GSK, Merck, and Pfizer, Inc., and honoraria from Pediatric News. Rangaraj Selvarangan reports grants from Hologic, BioFire Diagnostics, Becton Dickinson, Luminex, and Cepheid and serves on the GSK advisory board. Geoffrey A. Weinberg reports consulting fees from ReViral and honoraria from Merck for writing textbook chapters in the Merck Manual. John V. Williams reports grant support from the National Institutes of Health (for work unrelated to the report), consulting fees from Quidel’s scientific advisory board, and honorarium from the Infectious Disease of Children for a conference presentation, participation on a GSK independent data monitoring committee and on a data safety monitoring board for the National Institute of Allergy and Infectious Diseases IMPAACT Study. No other potential conflicts of interest were disclosed.
Figures
References
-
- Iwane MK, Edwards KM, Szilagyi PG, et al. ; New Vaccine Surveillance Network. Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children. Pediatrics 2004;113:1758–64. 10.1542/peds.113.6.1758 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
