

Evolution of antithrombotic therapy for patients with atrial fibrillation: The prospective global GLORIA-AF registry program
- PMID: 36201473
- PMCID: PMC9536607
- DOI: 10.1371/journal.pone.0274237
Evolution of antithrombotic therapy for patients with atrial fibrillation: The prospective global GLORIA-AF registry program
Abstract
Objective: To assess baseline characteristics and antithrombotic treatment (ATT) prescription patterns in patients enrolled in the third phase of the GLORIA-AF Registry Program, evaluate predictors of treatment prescription, and compare results with phase II.
Methods: GLORIA-AF is a large, global, prospective registry program, enrolling patients with newly diagnosed nonvalvular atrial fibrillation (AF) at risk of stroke. Patients receiving dabigatran were followed for two years in phase II, and all patients were followed for 3 years in phase III. Phase II started when dabigatran became available; phase III started when the characteristics of patients receiving dabigatran became roughly comparable with those receiving vitamin K antagonists (VKAs).
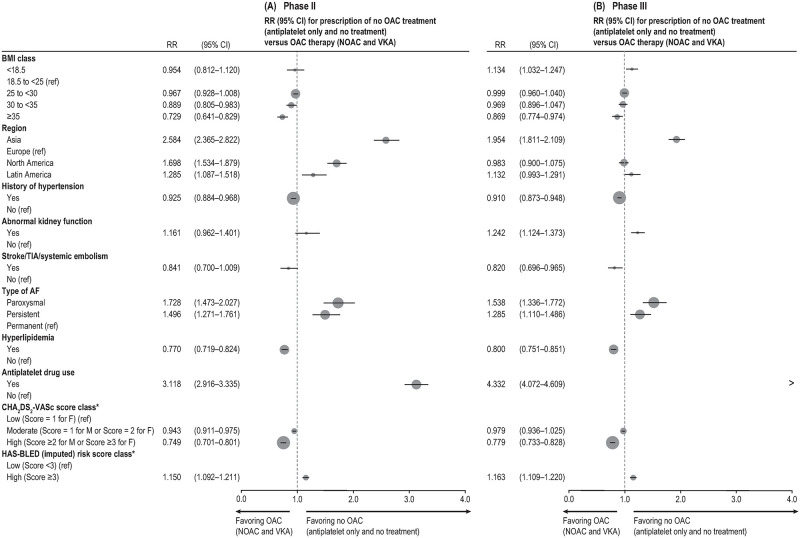
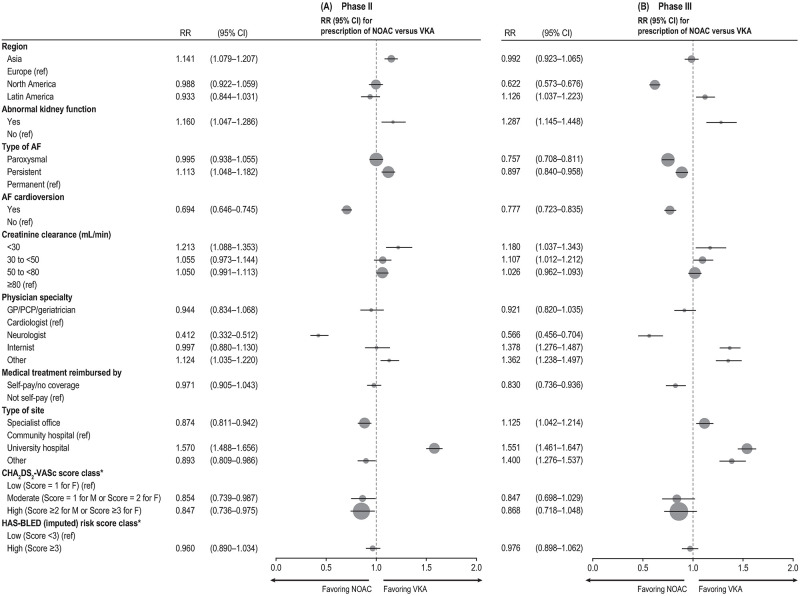
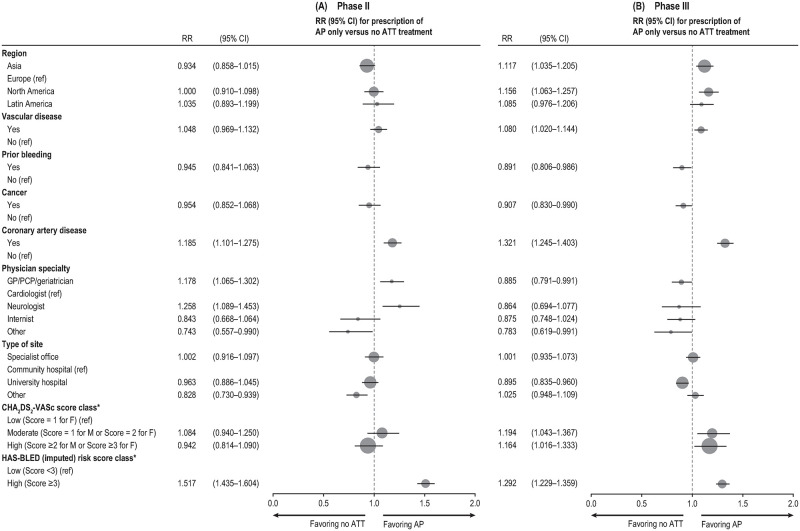
Results: Between 2014 and 2016, 21,241 patients were enrolled in phase III. In total, 82% of patients were prescribed oral anticoagulation ([OAC]; 59.5% novel/nonvitamin K oral anticoagulants [NOACs], 22.7% VKAs). A further 11% of patients were prescribed antiplatelets without OAC and 7% were prescribed no ATT. A high stroke risk was the main driver of OAC prescription. Factors associated with prescription of VKA over NOAC included type of site, region, physician specialty, and impaired kidney function.
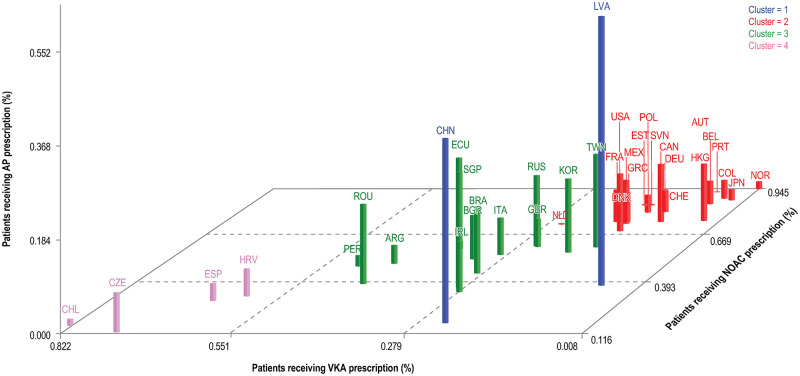
Conclusion: Over the past few years, data from phase III of GLORIA-AF show that OACs have become the standard treatment option, with most newly diagnosed AF patients prescribed a NOAC. However, in some regions a remarkable proportion of patients remain undertreated. In comparison with phase II, more patients received NOACs in phase III while the prescription of VKA decreased. VKAs were preferred over NOACs in patients with impaired kidney function.
Conflict of interest statement
L Beier declares no conflicts of interest at the time of manuscript writing and is now an employee of Novartis Pharma GmbH. S Lu was an employee of Boehringer Ingelheim at the time of manuscript writing and is now employed by Biogen Inc. S Marler, C Teutsch, K Zint, L Baker and M Paquette are employees of Boehringer Ingelheim. L Riou França was an employee of Boehringer Ingelheim at the time of manuscript writing and is now employed by Sanofi-Aventis. GYH Lip is a consultant and speaker for BMS/Pfizer, Boehringer Ingelheim and Daiichi-Sankyo. No fees are received personally. MV Huisman reports grants from ZonMW Dutch Healthcare Fund, grants and fees to the hospital from Boehringer Ingelheim, Pfizer-BMS, Bayer HealthCare, Aspen, Daiichi-Sankyo, outside the submitted work. JL Halperin has engaged in consulting activities with Boehringer Ingelheim, for advisory activities involving anticoagulants, and he is a member of the Executive Steering Committee of the GLORIA-AF Registry. H-C Diener has received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Abbott, Bayer Vital, Bristol-Myers Squibb (BMS), Boehringer Ingelheim, Daiichi-Sankyo, Medtronic, Pfizer, Portola, Sanofi-Aventis, and WebMD Global. Financial support for research projects was provided by Boehringer Ingelheim. Dr Diener chairs the Treatment Guidelines Committee of the German Society of Neurology and contributed to the EHRA and ESC guidelines for the treatment of AF. C-S Ma has received honoraria for lectures from AstraZeneca, Bayer HealthCare, Boehringer Ingelheim, BMS, Johnson & Johnson, and Pfizer. DB Bartels was an employee of Boehringer Ingelheim at time of manuscript writing and is now an employee at UCB Pharma GmbH. SJ Dubner has received consultancy fees for serving as a steering committee member for Boehringer Ingelheim; he also holds research grants from St Jude Medical. P Lyrer has received honoraria for contribution to advisory boards from Boehringer Ingelheim, BMS, Bayer, Pfizer, Daiichi Sankyo, and Ricordati, and research grants from the Swiss Heart Foundation, Swiss National Foundation, Bayer, Sanofi, Acticor, and the University Hospital Basel foundation (propatient). J Senges has received honoraria for contribution to advisory boards from Boehringer Ingelheim. KJ Rothman declares no conflicts of interest.
Figures
Similar articles
-
Antithrombotic Treatment Patterns in Patients with Newly Diagnosed Nonvalvular Atrial Fibrillation: The GLORIA-AF Registry, Phase II.Am J Med. 2015 Dec;128(12):1306-13.e1. doi: 10.1016/j.amjmed.2015.07.013. Epub 2015 Aug 1. Am J Med. 2015. PMID: 26239094
-
The Changing Landscape for Stroke Prevention in AF: Findings From the GLORIA-AF Registry Phase 2.J Am Coll Cardiol. 2017 Feb 21;69(7):777-785. doi: 10.1016/j.jacc.2016.11.061. J Am Coll Cardiol. 2017. PMID: 28209218
-
Antithrombotic therapy use in patients with atrial fibrillation before the era of non-vitamin K antagonist oral anticoagulants: the Global Registry on Long-Term Oral Antithrombotic Treatment in Patients with Atrial Fibrillation (GLORIA-AF) Phase I cohort.Europace. 2016 Sep;18(9):1308-18. doi: 10.1093/europace/euw073. Epub 2016 Jun 21. Europace. 2016. PMID: 27335063 Free PMC article.
-
Non-vitamin K antagonist oral anticoagulants in cardiovascular disease management: evidence and unanswered questions.J Clin Pharm Ther. 2014 Apr;39(2):118-35. doi: 10.1111/jcpt.12122. Epub 2014 Jan 3. J Clin Pharm Ther. 2014. PMID: 24383983 Review.
-
Clinical Performance of Nonvitamin K Antagonist Oral Anticoagulants in Real-World Obese Patients with Atrial Fibrillation.Semin Thromb Hemost. 2020 Nov;46(8):970-976. doi: 10.1055/s-0040-1715792. Epub 2020 Oct 26. Semin Thromb Hemost. 2020. PMID: 33105504 Review.
Cited by
-
How the Hemostasis Laboratory Can Help Clinicians to Manage Patients on Oral Anticoagulants.Mediterr J Hematol Infect Dis. 2024 Mar 1;16(1):e2024027. doi: 10.4084/MJHID.2024.027. eCollection 2024. Mediterr J Hematol Infect Dis. 2024. PMID: 38468834 Free PMC article. Review.
-
Real world time trends in antithrombotic treatment for newly diagnosed atrial fibrillation in China: reports from the GLORIA-AF Phase III registry : Trends in antithrombotic therapy use in China.Thromb J. 2023 Aug 1;21(1):83. doi: 10.1186/s12959-023-00527-x. Thromb J. 2023. PMID: 37528405 Free PMC article.
-
Community-based analysis of stroke prevention and effect of public interventions in atrial fibrillation: results from the ARENA project.Clin Res Cardiol. 2025 Jan;114(1):138-149. doi: 10.1007/s00392-024-02510-6. Epub 2024 Aug 8. Clin Res Cardiol. 2025. PMID: 39115608 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
