

Spine and lower body symmetry during treadmill walking in healthy individuals-In-vivo 3-dimensional kinematic analysis
- PMID: 36201499
- PMCID: PMC9536630
- DOI: 10.1371/journal.pone.0275174
Spine and lower body symmetry during treadmill walking in healthy individuals-In-vivo 3-dimensional kinematic analysis
Abstract
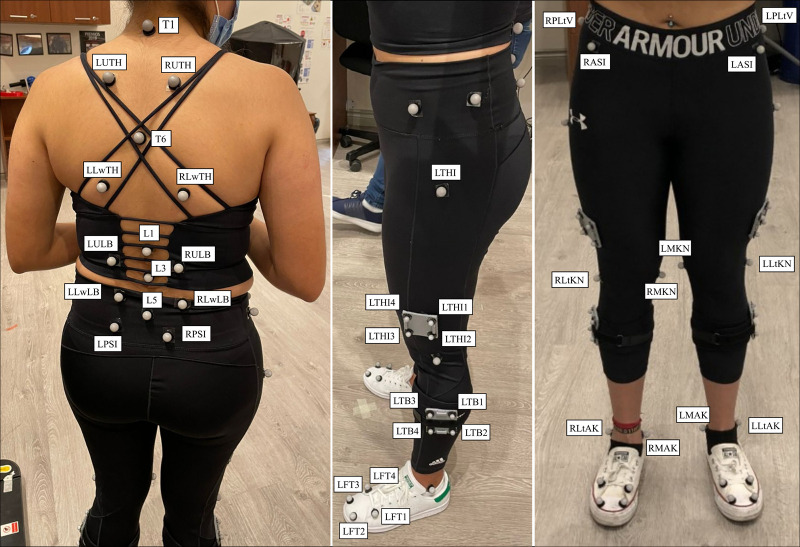
Although it is relevant to understand spine and lower body motions in healthy individuals for a variety of applications, such as clinical diagnosis, implant design, and the analysis of treatment outcomes, proper assessment and characterization of normative gait symmetry in healthy individuals remains unclear. The purpose of this study was to investigate the in vivo 3-dimensional (3D) spine and lower body gait symmetry kinematics during treadmill walking in healthy individuals. Sixty healthy young adults (30 males and 30 females) were evaluated during normal and fast treadmill walking using a motion capture system approach. Statistical parametric mapping and the normalized symmetry index approaches were used to determine spine, pelvis, and lower body asymmetries during treadmill walking. The spine and pelvis angular motions associated with the left and right lower limb motions, as well as the left and right lower extremity joint angles were compared for normal and fast treadmill walking. The lower lumbar left-right rotation (5.74±0.04°) and hip internal rotation (5.33±0.18°) presented the largest degrees of asymmetry during normal treadmill. Upper lumbar left-right lateral flexion (1.48±0.14°) and knee flexion (2.98±0.13°) indicated the largest asymmetries and during fast treadmill walking. Few asymmetry patterns were similar between normal and fast treadmill walking, whereas others appeared either only during normal or fast treadmill walking in this cohort of participants. These findings could provide insights into better understanding gait asymmetry in healthy individuals, and use them as reference indicators in diagnosing and evaluating abnormal gait function.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Sadeghisani M, Manshadi FD, Kalantari KK, Rahimi A, Namnik N, Karimi MT, et al. Correlation between Hip Rotation Range-of-Motion Impairment and Low Back Pain. A Literature Review. Ortopedia, traumatologia, rehabilitacja. 2015;17(5):455–62. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
