

Risk of retinal detachment and exposure to fluoroquinolones, common antibiotics, and febrile illness using a self-controlled case series study design: Retrospective analyses of three large healthcare databases in the US
- PMID: 36201545
- PMCID: PMC9536641
- DOI: 10.1371/journal.pone.0275796
Risk of retinal detachment and exposure to fluoroquinolones, common antibiotics, and febrile illness using a self-controlled case series study design: Retrospective analyses of three large healthcare databases in the US
Abstract
Objective: The risk of retinal detachment (RD) following exposure to fluoroquinolone (FQ) has been assessed in multiple studies, however, results have been mixed. This study was designed to estimate the risk of RD following exposure to FQ, other common antibiotics, and febrile illness not treated with antibiotics (FINTA) using a self-controlled case series (SCCS) study design to reduce risk of confounding from unreported patient characteristics.
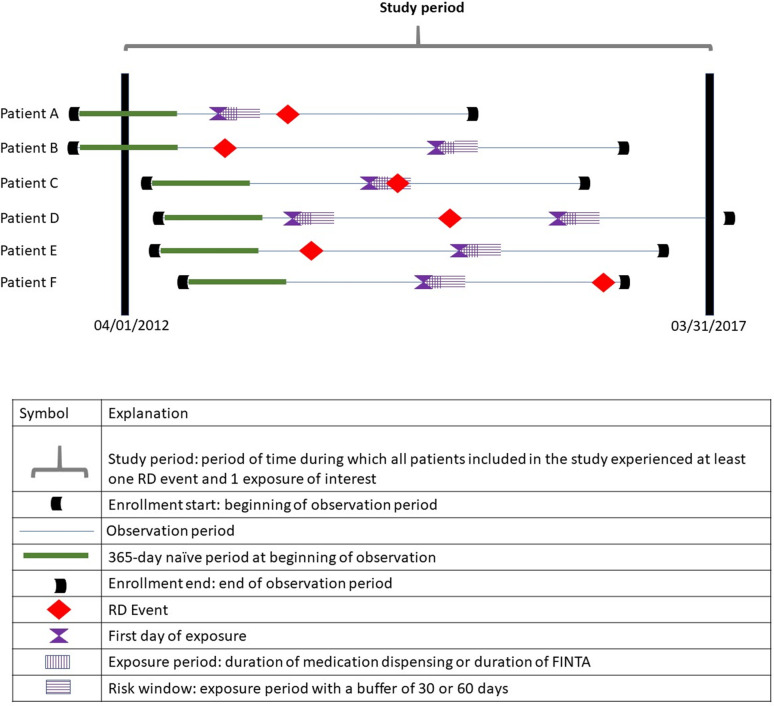
Design: Retrospective database analysis-SCCS.
Setting: Primary and Secondary Care.
Study population: 40,981 patients across 3 US claims databases (IBM® MarketScan® commercial and Medicare databases, Optum Clinformatics).
Outcome: RD.
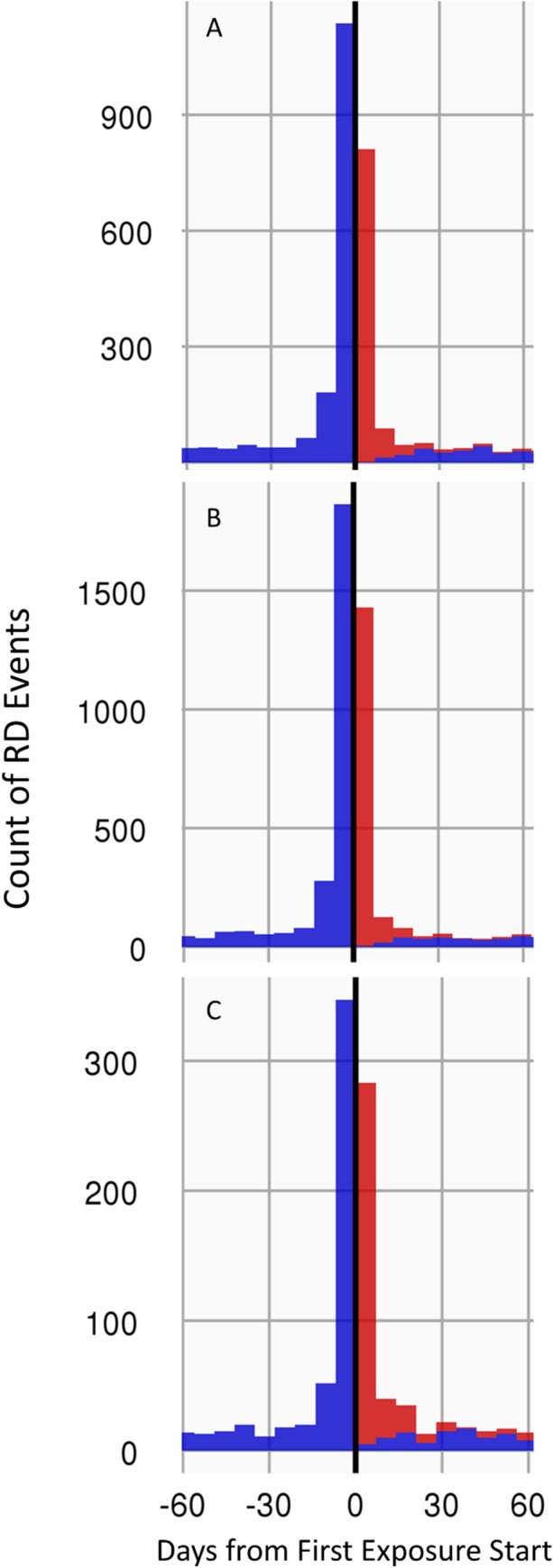
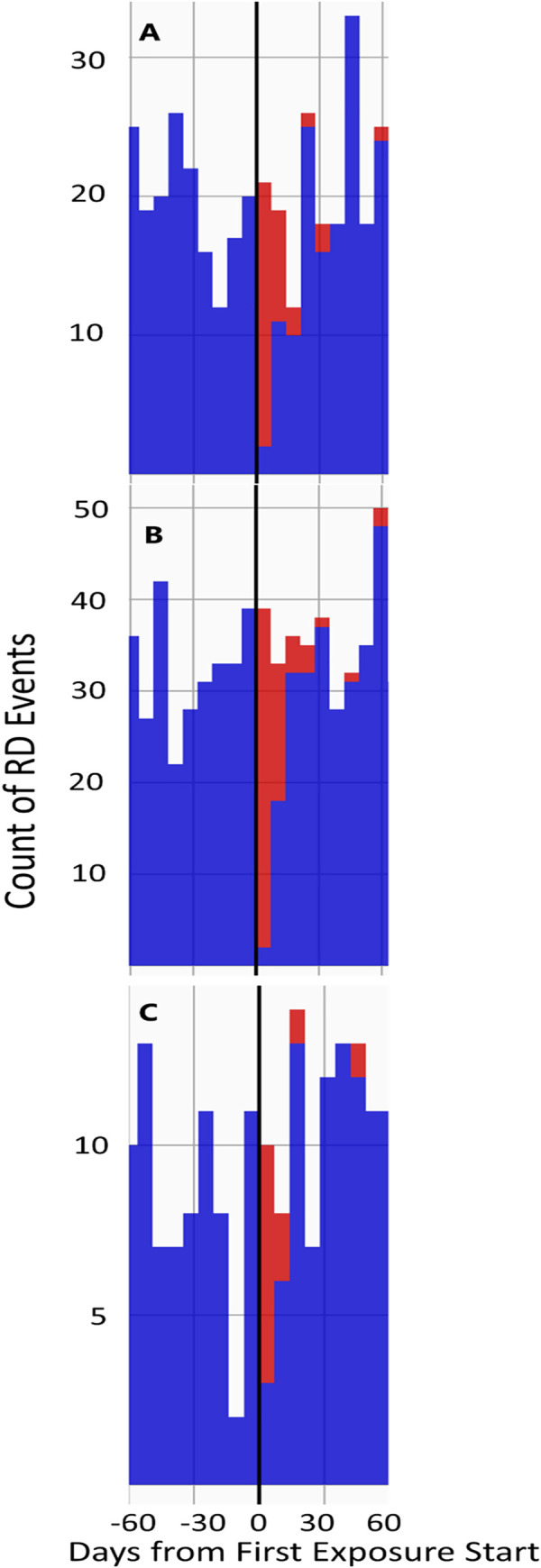
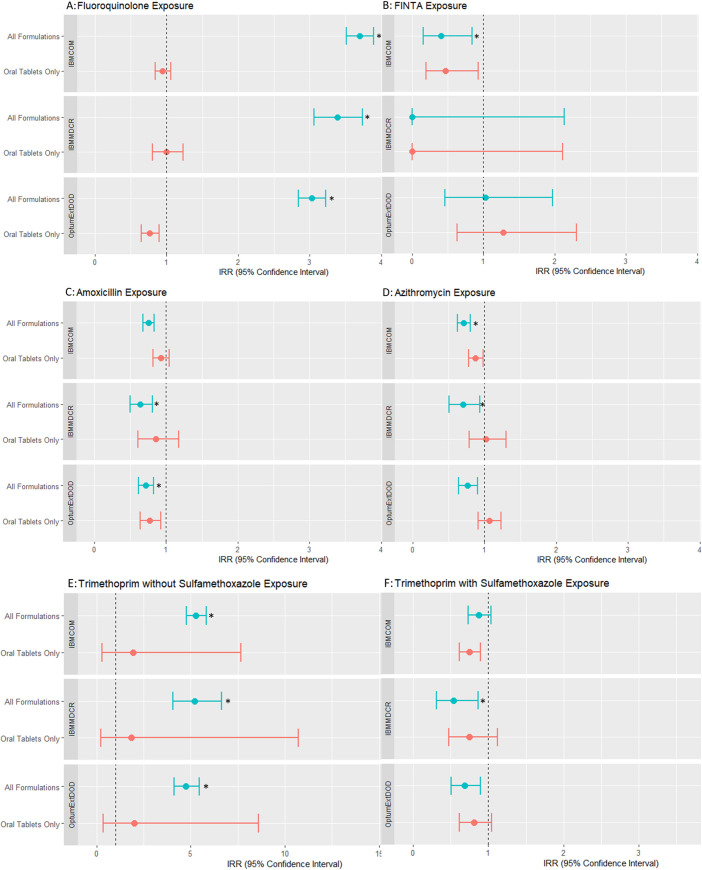
Methods: Exposures included FQ as a class of drugs, amoxicillin, azithromycin, trimethoprim with and without sulfamethoxazole, and FINTA. For the primary analysis, all drug formulations were included. For the post hoc sensitivity analyses, only oral tablets were included. Risk windows were defined as exposure period (or FINTA duration) plus 30 days. Patients of all ages with RD and exposures in 3 US claims databases between 2012 to 2017 were included. Diagnostics included p value calibration and pre-exposure outcome analyses. Incidence rate ratios (IRR) and 95% confidence interval (CI) comparing risk window time with other time were calculated.
Results: Our primary analysis showed an increased risk for RD in the 30 days prior to exposure to FQ or trimethoprim without sulfamethoxazole. This risk decreased but remained elevated for 30 days following first exposure. Our post-hoc analysis, which excluded ophthalmic drops, showed no increased risk for RD at any time, with FQ and other antibiotics.
Conclusion: Our results did not suggest an association between FQ and RD. Oral FQ was not associated with an increased risk for RD during the pre- or post-exposure period.
Trial registration: ClinicalTrials.gov identifier: NCT03479736-March 21, 2018.
Conflict of interest statement
At the time of the work, all authors were full-time employees of Janssen Research & Development, LLC, which is the Marketing Authorisation Holder for Levaquin (a fluoroquinolone) in the United States and some other countries. As full-time employees, the authors held stock or stock options. This does not alter the authors’ adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Li X. and G. Beijing Rhegmatogenous Retinal Detachment Study, Incidence and epidemiological characteristics of rhegmatogenous retinal detachment in Beijing, China. Ophthalmology, 2003. 110(12): p. 2413–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
