

Comparative Analysis of Robotics-Assisted and Manual Insertions of Cochlear Implant Electrode Arrays
- PMID: 36201552
- PMCID: PMC10962863
- DOI: 10.1097/MAO.0000000000003707
Comparative Analysis of Robotics-Assisted and Manual Insertions of Cochlear Implant Electrode Arrays
Abstract
Hypothesis: Robotics-assisted cochlear implant (CI) insertions will result in reduced intracochlear trauma when compared with manual, across multiple users.
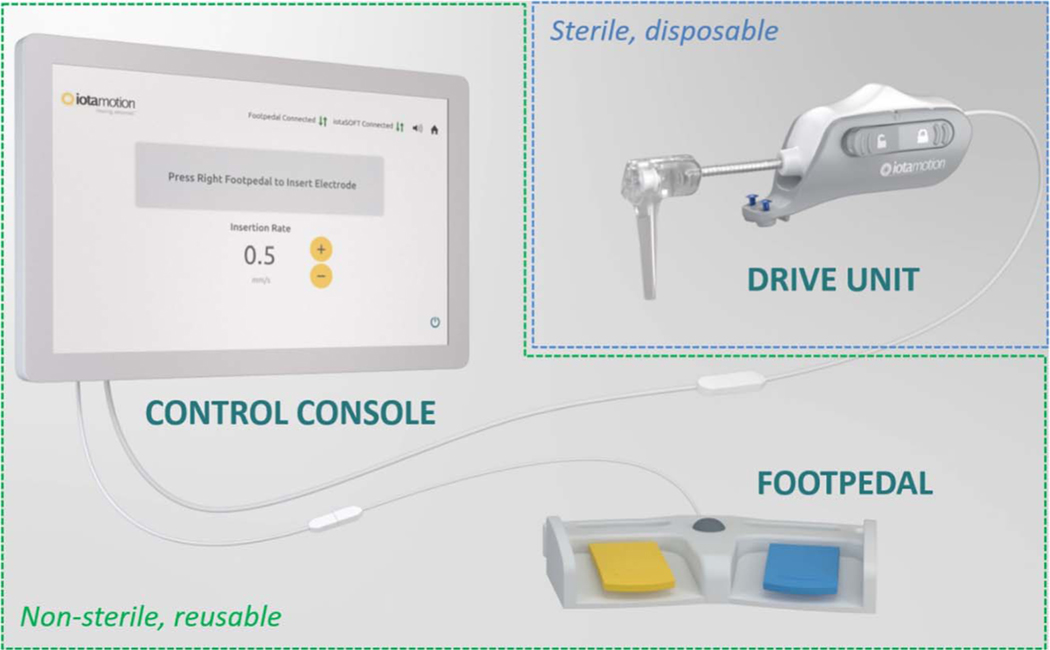
Background: Whether intracochlear trauma and translocations are two factors that may contribute to significant variability in CI outcomes remains to be seen. To address this issue, we have developed a robotics-assisted insertion system designed to aid the surgeon in inserting electrode arrays with consistent speeds and reduced variability. This study evaluated the effect of robotics-assisted insertions on the intracochlear trauma as compared with manual insertions in cadaveric cochleae in a simulated operative environment.
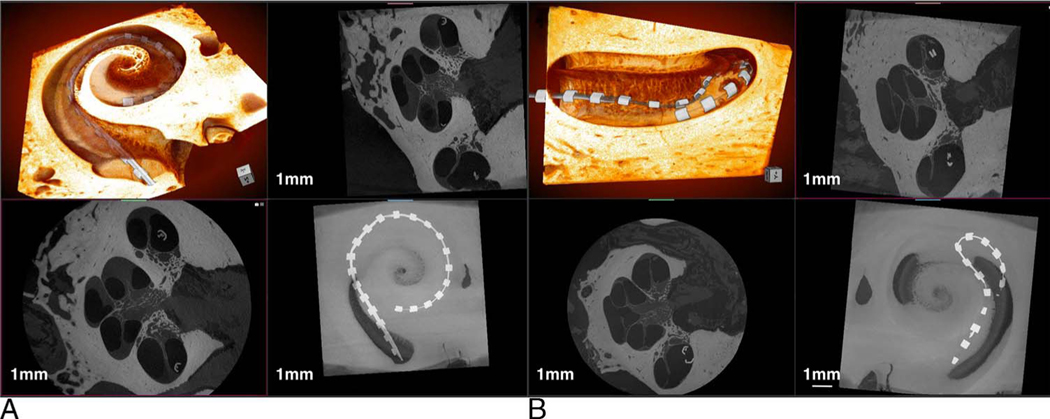
Methods: Twelve neurotologists performed bilateral electrode insertions into cochleae of full cadaveric heads using both the robotics-assisted system and manual hand insertion. Lateral wall electrodes from three different manufacturers (n = 24) were used and randomized between surgeons. Insertion angle of the electrode and trauma scoring were evaluated using high-resolution three-dimensional x-ray microscopy and compared between robotics-assisted and manual insertions.
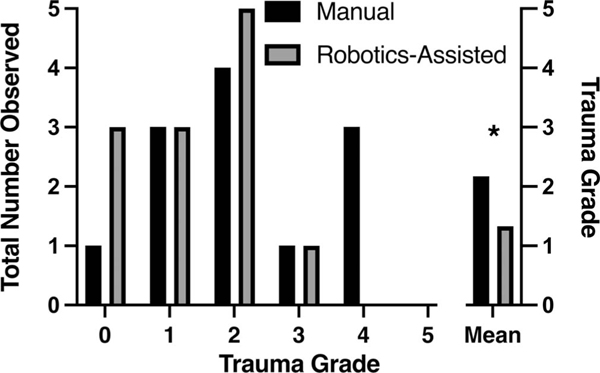
Results: Three-dimensional x-ray microscopy provided excellent resolution to characterize the in situ trauma and insertion angle. Robotics-assisted insertions significantly decreased insertional intracochlear trauma as measured by reduced trauma scores compared with manual insertions (average: 1.3 versus 2.2, device versus manual, respectively; p < 0.05). There was no significant difference between insertion angles observed for manual and robotics-assisted techniques (311 ± 131° versus 307 ± 96°, device versus manual, respectively).
Conclusions: Robotics-assisted insertion systems enable standardized electrode insertions across individual surgeons and experience levels. Clinical trials are necessary to investigate whether insertion techniques that reduce insertional variability and the likelihood of intracochlear trauma also improve CI auditory outcomes.
Copyright © 2022, Otology & Neurotology, Inc.
Conflict of interest statement
Sources of support and disclosure of funding: C.R.K. and M.R.H. are co-founders and directors of iotaMotion, Inc. A.H. is an iotaMotion employee. For the remaining authors, there are no conflicts of interest to report. Funding was provided by iotaMotion, Inc., and the National Institute on Deafness and Other Communication Disorders (T32 DC00040).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
