

Outcomes With Local Therapy and Tyrosine Kinase Inhibition in Patients With ALK/ ROS1/ RET-Rearranged Lung Cancers
- PMID: 36201714
- PMCID: PMC9848570
- DOI: 10.1200/PO.22.00024
Outcomes With Local Therapy and Tyrosine Kinase Inhibition in Patients With ALK/ ROS1/ RET-Rearranged Lung Cancers
Abstract
Purpose: Local therapy prolongs progression-free survival in patients with oligometastatic non-small-cell lung cancers treated with chemotherapy. We previously reported that local therapy also prolongs survival and time to next therapy in patients on tyrosine kinase inhibitors (TKIs) for EGFR-mutant lung adenocarcinomas. Here, we investigate the role of local therapy in patients progressing on TKIs for ALK/ROS1/RET-rearranged lung adenocarcinomas.
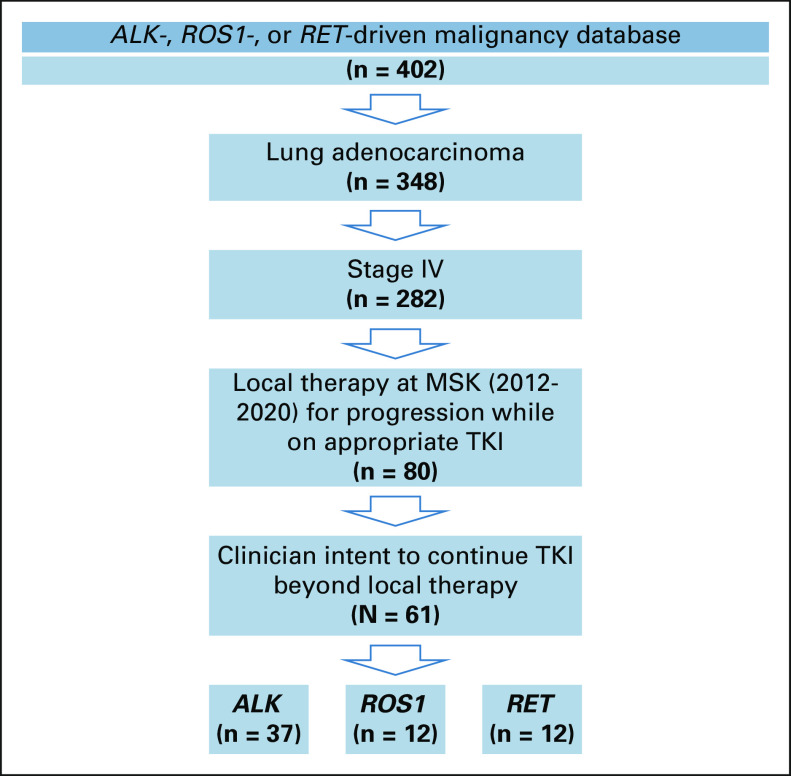
Materials and methods: Patients with advanced ALK/ROS/RET-rearranged lung adenocarcinomas who underwent radiation, surgery, or percutaneous thermal ablation from 2012 to 2020 for progression on an ALK/ROS1/RET TKI were included. Progression patterns were identified. Times from local therapy to progression, next therapy, and death were measured.
Results: Sixty-one patients with ALK (n = 37), ROS1 (n = 12), and RET (n = 12) fusions were identified. Patients received radiotherapy (92%), surgery (13%), and percutaneous thermal ablation (8%). Local therapy was administered for solitary/oligoprogressive (94%) or polyprogressive (6%) disease. For most patients (85%), local therapy addressed all progressing sites. The median times from any local therapy to subsequent progression and next systemic therapy were 6.8 months (95% CI, 5.1 to 8.1) and 10 months (95% CI, 8.4 to 15.3), respectively. Third or greater local therapy was associated with shorter time to progression and next therapy than first/second local therapies (hazard ratio, 4.97; P < .001 and hazard ratio, 2.48; P < .001). The median overall survival from first local therapy was 34 months (95% CI, 26 to not reached).
Conclusion: Local therapy for progression on ALK, ROS1, or RET TKIs is associated with clinically meaningful time on continued TKI therapy beyond progression, especially earlier in the course of disease.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Honoraria: Pfizer, Loxo/Bayer/Lilly, IASLC, Helsinn Therapeutics, BeiGene, Remedica, TP Therapeutics, Verastem, AstraZeneca, Ignyta/Genetech/Roche, Liberum, Lungevity, NIH, PER, OncLive/MJH Life Sciences, Clinical Care Options/NCCN, Lung Cancer Research Foundation, Associazione Italiana Oncologia Toracica (AIOT), Chugai Pharma, Sirio Libanes Hospital, Answers in CME, Research to Practice, RV More, i3 Health
No other potential conflicts of interest were reported.
Figures



References
-
- Peters S, Camidge DR, Shaw AT, et al. : Alectinib versus crizotinib in untreated ALK-positive non-small-cell lung cancer. N Engl J Med 377:829-838, 2017 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
