

Fluid Overload and Precision Net Ultrafiltration in Critically Ill Patients
- PMID: 36202071
- PMCID: PMC10076441
- DOI: 10.1159/000527390
Fluid Overload and Precision Net Ultrafiltration in Critically Ill Patients
Abstract
Background: Fluid overload is present in two-thirds of critically ill patients with acute kidney injury and is associated with morbidity, mortality, and increased healthcare resource utilization. Kidney replacement therapy (KRT) is frequently used for net fluid removal (i.e., net ultrafiltration [UFNET]) in patients with severe oliguric acute kidney injury. However, ultrafiltration has considerable risks associated with it, and there is a need for newer technology to perform ultrafiltration safely and to improve outcomes.
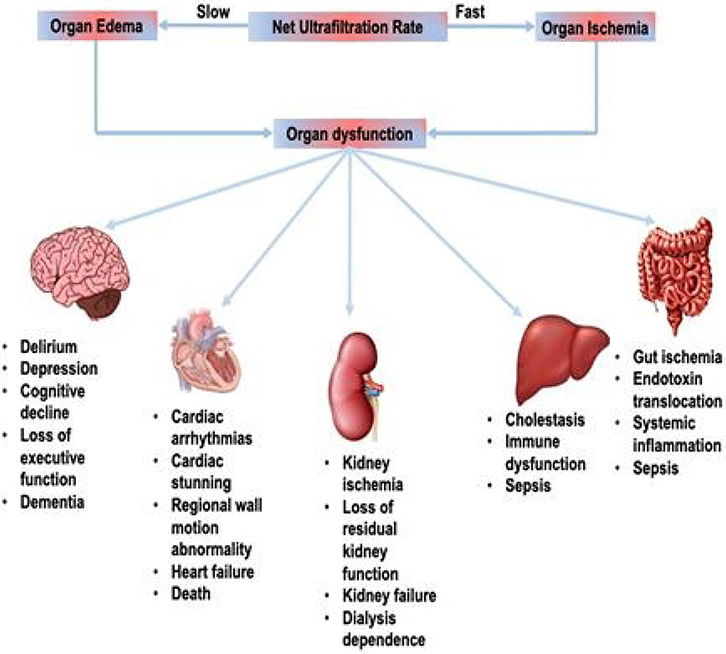
Summary: Caring for a critically ill patient with oliguric acute kidney injury and fluid overload is one of the most challenging problems. Although diuretics are the first-line treatment for management of fluid overload, diuretic resistance is common. Various clinical practice guidelines support fluid removal using ultrafiltration during KRT. Emerging evidence from observational studies in critically ill patients suggests that both slow and fast rates of net fluid removal during continuous kidney replacement therapy are associated with increased mortality compared with moderate UFNET rates. In addition, fast UFNET rates are associated with an increased risk of cardiac arrhythmias. Randomized trials are required to examine whether moderate UFNET rates are associated with a reduced risk of hemodynamic instability, organ injury, and improved outcomes in critically ill patients. There is a need for newer technology for fluid removal in patients who do not meet traditional criteria for initiation of KRT. Emerging newer and miniaturized ultrafiltration devices may address an unmet clinical need.
Key messages: Among critically ill patients with acute kidney injury and fluid overload requiring continuous kidney replacement therapy, use of higher and slower UFNET rates compared with moderate UFNET rates might be associated with poor outcomes. Newer minimally invasive technologies may allow for safe and efficient UFNET in patients with acute kidney injury who do not meet criteria for initiation of KRT.
Keywords: Fluid overload; Kidney replacement therapy; Mortality; Net ultrafiltration.
© 2022 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Conflict of Interest Statement
Dr. Raghavan Murugan reported receiving grants and personal fees from La Jolla Inc.; grants from Bioporto, Inc. and the National Institute of Diabetes and Digestive and Renal Diseases; personal fees from Beckman Coulter, and AM Pharma, Inc.; and consulting fee from Baxter outside the submitted work. Dr. Claudio Ronco reported receiving consulting fees or participating in advisory boards in the last 3 years for ASAHI, Astute, Baxter, Biomerieux, B. Braun, Cytosorbents, ESTOR, FMC, GE, Jafron, Medtronic, and Toray.
Figures

References
-
- Murugan R, Bellomo R, Palevsky PM, Kellum JA. Ultrafiltration in critically ill patients treated with kidney replacement therapy. Nat Rev Nephrol. 2021. Apr;17(4):262–76. - PubMed
-
- Rosner MH, Ostermann M, Murugan R, Prowle JR, Ronco C, Kellum JA, et al. Indications and management of mechanical fluid removal in critical illness. Br J Anaesth. 2014. Nov;113(5):764–71. - PubMed
-
- Messmer AS, Zingg C, Muller M, Gerber JL, Schefold JC, Pfortmueller CA. Fluid Overload and Mortality in Adult Critical Care Patients-A Systematic Review and Meta-Analysis of Observational Studies. Crit Care Med. 2020. Dec;48(12):1862–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
