

Chronic liver disease and hepatic calcium-oxalate deposition in patients with primary hyperoxaluria type I
- PMID: 36202824
- PMCID: PMC9537520
- DOI: 10.1038/s41598-022-19584-9
Chronic liver disease and hepatic calcium-oxalate deposition in patients with primary hyperoxaluria type I
Abstract
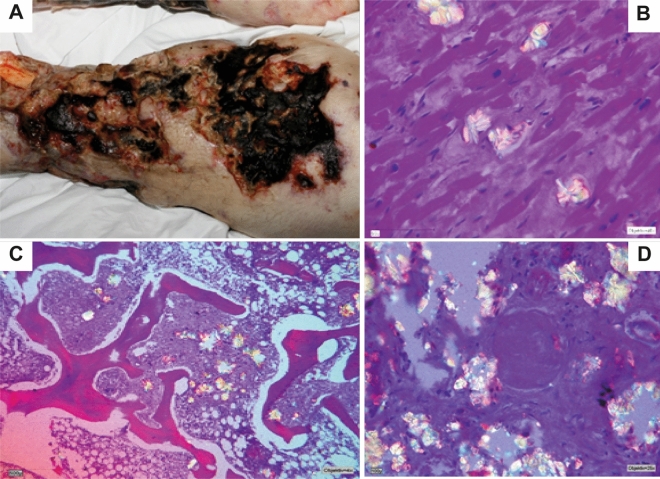
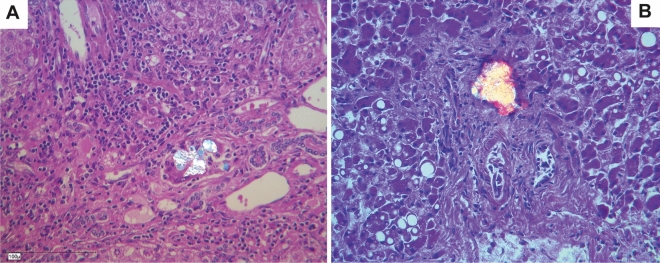
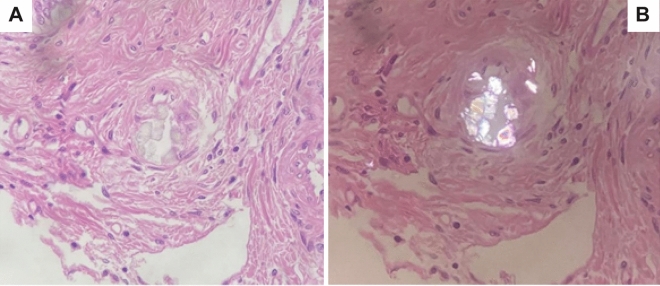
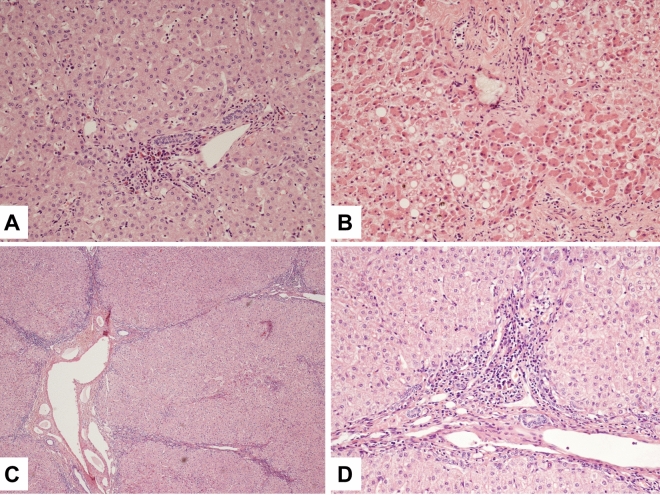
Patients with primary hyperoxaluria type I (PH I) are prone to develop early kidney failure. Systemic deposition of calcium-oxalate (CaOx) crystals starts, when renal function declines and plasma oxalate increases. All tissue, but especially bone, heart and eyes are affected. However, liver involvement, as CaOx deposition or chronic hepatitis/fibrosis has never been reported. We examined liver specimen from 19 PH I patients (aged 1.5 to 52 years at sample collection), obtained by diagnostic biopsy (1), at autopsy (1), or transplantation (17). With polarization microscopy, birefringent CaOx crystals located in small arteries, but not within hepatocytes were found in 3/19 patients. Cirrhosis was seen in one, fibrosis in 10/19 patients, with porto-portal and nodular fibrosis (n = 1), with limitation to the portal field in 8 and/or to central areas in 5 patients. Unspecific hepatitis features were observed in 7 patients. Fiber proliferations were detectable in 10 cases and in one sample transformed Ito-cells (myofibroblasts) were found. Iron deposition, but also megakaryocytes as sign of extramedullary erythropoiesis were found in 9, or 3 patients, respectively. Overall, liver involvement in patients with PH I was more pronounced, as previously described. However, CaOx deposition was negligible in liver, although the oxalate concentration there must be highest.
© 2022. The Author(s).
Conflict of interest statement
CMH is a consultant of Dicerna a NovoNordisk subsidiary, USA/Denmark. BBB received consulting fees from Alnylam Pharmaceuticals, USA. BH has been an employee of Dicerna a NovoNordisk subsidiary, USA/Denmark. The other authors have nothing to declare.
Figures
References
-
- Lorenzo V, Torres A, Salido E. Primary hyperoxaluria. Nefrologia Publicacion Oficial de la Sociedad Espanola Nefrologia. 2014;34:398–412. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
