

Clinical outcomes and treatment patterns of older adults with dementia-related psychosis by dementia type in the United States
- PMID: 36203129
- PMCID: PMC9541053
- DOI: 10.1186/s12877-022-03489-3
Clinical outcomes and treatment patterns of older adults with dementia-related psychosis by dementia type in the United States
Abstract
Background: Little is known about the incidence of clinical events and treatment patterns among older adults with dementia-related psychosis. Given that dementia-related psychosis comprises various dementia types, this study describes the incidence of clinical events and treatment patterns by dementia type after patients with dementia are diagnosed with psychosis.
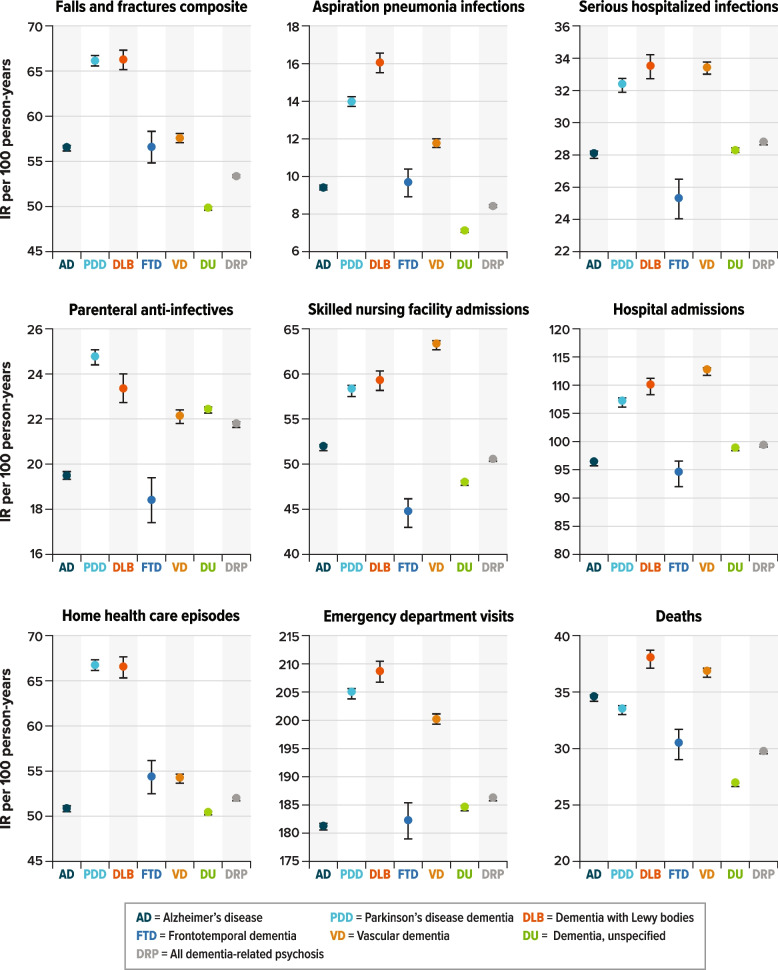
Methods: Adults aged ≥ 65 years with dementia and newly diagnosed with psychosis were identified in US Medicare claims during 2013-2018. Baseline characteristics were evaluated at the time of the psychosis diagnosis. After the initial psychosis diagnosis, incidence rates (IRs) of clinical events (e.g., falls/fractures, infections, healthcare utilization), mortality, and patterns of antipsychotic treatment were described for each dementia type (Alzheimer's disease [AD], Parkinson's disease dementia [PDD], dementia with Lewy bodies [DLB], frontotemporal dementia [FTD], vascular dementia [VD], and unspecified dementia). Daily mean cumulative counts were estimated to describe the incidence of recurrent events over time. Mortality was described using Kaplan-Meier survival curves.
Results: We identified 484,520 patients with dementia-related psychosis: mean age, 84 years (standard deviation, 7.8); female, 66%. At the time of psychosis diagnosis, the most prevalent type of dementia was unspecified dementia (56%), followed by AD (31%), VD (12%), PDD (10%), DLB (3%), and FTD (< 1%), and most patients had scores indicating severe illness on the Charlson Comorbidity Index (71%) and frailty index (62%). Across all dementia types, IRs (per 100 person-years) were high for emergency department visits, oral anti-infective use, and urinary tract infections after the initial psychosis diagnosis. Patients with DLB had the highest incidence of most clinical outcomes. After 1 year of follow-up, the cumulative probability of death was about 30% for all dementia types, and after 5 years, was about 80% among patients with DLB, VD, AD, or PDD and about 60%-65% among patients with FTD or unspecified dementia.
Conclusions: Patients with dementia-related psychosis had a high burden of comorbidities, frailty, emergency department visits, infections, and death. Specifically, after DRP diagnosis, patients with DLB and VD had the highest burden of clinical events of interest.
Keywords: Alzheimer’s disease; Antipsychotics; Dementia with Lewy bodies; Frontotemporal dementia; Healthcare utilization; Infections; Medicare; Mortality; Parkinson’s disease dementia; Vascular dementia.
© 2022. The Author(s).
Conflict of interest statement
MET and CD are employees of Acadia Pharmaceuticals, which produces an antipsychotic treatment. GD was an employee of Acadia Pharmaceuticals at the time this work was conducted. JF, HED, LJM, MSA and JBL are employees of RTI Health Solutions. This study was conducted by RTI Health Solutions with funding from Acadia Pharmaceuticals under a contract that included independent publication rights.
Figures


References
-
- Marcinkowska M, Sniecikowska J, Fajkis N, Pasko P, Franczyk W, Kolaczkowski M. Management of dementia-related psychosis, agitation and aggression: a review of the pharmacology and clinical effects of potential drug candidates. CNS Drugs. 2020;34(3):243–268. doi: 10.1007/s40263-020-00707-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
