

Fertility-Sparing Approach in Patients with Endometrioid Endometrial Cancer Grade 2 Stage IA (FIGO): A Qualitative Systematic Review
- PMID: 36203482
- PMCID: PMC9532104
- DOI: 10.1155/2022/4070368
Fertility-Sparing Approach in Patients with Endometrioid Endometrial Cancer Grade 2 Stage IA (FIGO): A Qualitative Systematic Review
Abstract
Background: Endometrial cancer (EC) is one of the most common gynecologic malignancy, mostly in postmenopausal women. The gold standard treatment for EC is surgery, but in the early stages, it is possible to opt for conservative treatment. In the last decade, different clinical and pathological markers have been studied to identify women who respond to conservative treatment. A lot of immunohistochemical markers have been evaluated to predict response to progestin treatment, even if their usefulness is still unclear; the prognosis of this neoplasm depends on tumor stage, and a specific therapeutic protocol is set according to the stage of the disease.
Objective: (1) To provide an overview of the conservative management of Stage 1A Grade (G) 2 endometrioid EC (FIGO) and the oncological and reproductive outcomes related; (2) to describe the molecular alterations before and after progestin therapy in patients undergoing conservative treatment.
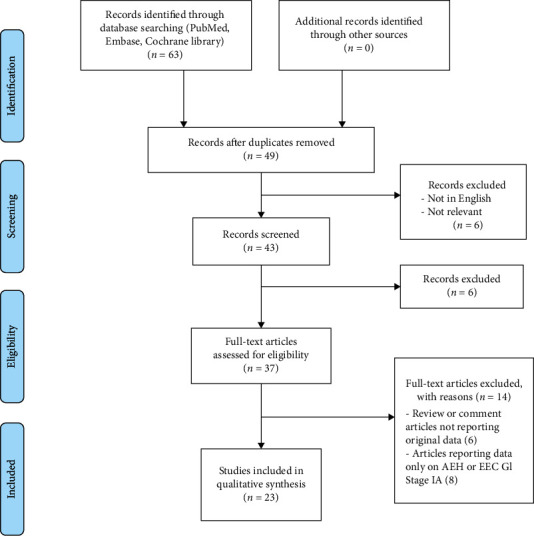
Materials and methods: A systematic computerized search of the literature was performed in the main electronic databases (MEDLINE, Embase, Web of Science, PubMed, and Cochrane Library), from 2010 to September 2021, in order to evaluate the oncological and reproductive outcomes in patients with G2 stage IA EC who ask for fertility-sparing treatment. The expression of several immunohistochemical markers was evaluated in pretreatment phase and during the follow-up in relation to response to hormonal therapy. Only scientific publications in English were included. The risk of bias assessment was performed. Review authors' judgments were categorized as "low risk," "high risk," or "unclear risk" of bias.
Results: Twelve articles were included in the study: 7 observational studies and 5 case series/reports. Eighty-four patients who took progestins (megestrol acetate, medroxyprogesterone acetate, and/or levonorgestrel-releasing intrauterine devices) were analyzed. The publication bias analysis turned out to be "low." 54/84 patients had a complete response, 23/84 patients underwent radical surgery, and 20/84 had a relapse after conservative treatment. Twenty-two patients had a pregnancy. The length of follow-up was variable, from 6 to 142 months according to the different studies analyzed. Several clinical and pathological markers have been studied to identify women who do not respond to conservative treatment: PR and ER were the most studied predictive markers, in particular PR appeared as the most promising; MMR, SPAG9, Ki67, and Nrf2-survivin pathway provided good results with a significant association with a good response to progestin therapy. However, no reliable predictive markers are currently available to be used in clinical practice.
Conclusions: The conservative treatment may be an option for patients with stage IA G2 EEC who desire to preserve their fertility. The immunohistochemical markers evaluation looks promising in predicting response to conservative treatment. Further large series and randomized clinical trials are needed to confirm these results.
Copyright © 2022 Pierluigi Giampaolino et al.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Fertility-preserving treatment for stage IA endometrial cancer: a systematic review and meta-analysis.Am J Obstet Gynecol. 2024 Dec;231(6):599-610.e17. doi: 10.1016/j.ajog.2024.07.018. Epub 2024 Jul 19. Am J Obstet Gynecol. 2024. PMID: 39032722
-
Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding.Cochrane Database Syst Rev. 2005 Oct 19;(4):CD002126. doi: 10.1002/14651858.CD002126.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2015 Apr 30;(4):CD002126. doi: 10.1002/14651858.CD002126.pub3. PMID: 16235297 Updated.
-
Pre-operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding.Cochrane Database Syst Rev. 2002;(3):CD001124. doi: 10.1002/14651858.CD001124. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2014 Jul 29;(7):CD001124. doi: 10.1002/14651858.CD001124.pub2. PMID: 12137619 Updated.
-
Hormone replacement therapy for women previously treated for endometrial cancer.Cochrane Database Syst Rev. 2018 May 15;5(5):CD008830. doi: 10.1002/14651858.CD008830.pub3. Cochrane Database Syst Rev. 2018. PMID: 29763969 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
Cited by
-
Unsolved Issues in the Integrated Histo-Molecular Classification of Endometrial Carcinoma and Therapeutic Implications.Cancers (Basel). 2024 Jul 4;16(13):2458. doi: 10.3390/cancers16132458. Cancers (Basel). 2024. PMID: 39001520 Free PMC article. Review.
-
Validation of a deep neural network-based algorithm supporting clinical management of adnexal mass.Front Med (Lausanne). 2023 Jan 23;10:1102437. doi: 10.3389/fmed.2023.1102437. eCollection 2023. Front Med (Lausanne). 2023. PMID: 36756174 Free PMC article.
-
Circulating miRNAs as a Tool for Early Diagnosis of Endometrial Cancer-Implications for the Fertility-Sparing Process: Clinical, Biological, and Legal Aspects.Int J Mol Sci. 2023 Jul 12;24(14):11356. doi: 10.3390/ijms241411356. Int J Mol Sci. 2023. PMID: 37511115 Free PMC article. Review.
-
Identification of lncRNAs associated with uterine corpus endometrial cancer prognosis based on the competing endogenous RNA network.Int J Med Sci. 2023 Sep 25;20(12):1600-1615. doi: 10.7150/ijms.87430. eCollection 2023. Int J Med Sci. 2023. PMID: 37859697 Free PMC article.
-
Coexistence of Primary Umbilical Endometriosis and Endometrial Hyperplasia: A Case Report and Review of the Literature.Int Med Case Rep J. 2023 May 31;16:323-328. doi: 10.2147/IMCRJ.S411149. eCollection 2023. Int Med Case Rep J. 2023. PMID: 37284434 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
