

Disrupted topological properties of the structural brain network in patients with cerebellar infarction on different sides are associated with cognitive impairment
- PMID: 36203973
- PMCID: PMC9530262
- DOI: 10.3389/fneur.2022.982630
Disrupted topological properties of the structural brain network in patients with cerebellar infarction on different sides are associated with cognitive impairment
Abstract
Purpose: To explore changes in the brain structural network in patients with cerebellar infarction on different sides and their correlations with changes in cognitive function.
Methods: Nineteen patients with acute left posterior cerebellar infarction and 18 patients with acute right posterior cerebellar infarction seen from July 2016 to September 2019 in the Department of Neurology, Affiliated Brain Hospital of Nanjing Medical University, were selected. A total of 27 healthy controls matched for sex, age, and years of education were recruited. The subjects underwent head diffusion magnetic resonance imaging examination and neuropsychological cognitive scale evaluation, and we analyzed changes in brain structural network properties in patients with cerebellar infarction and their correlation with changes in patients' cognitive function.
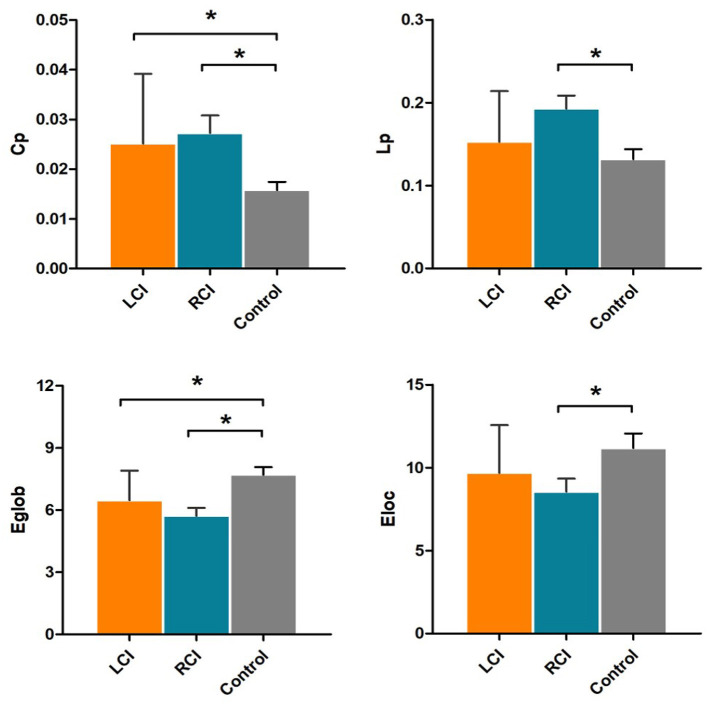
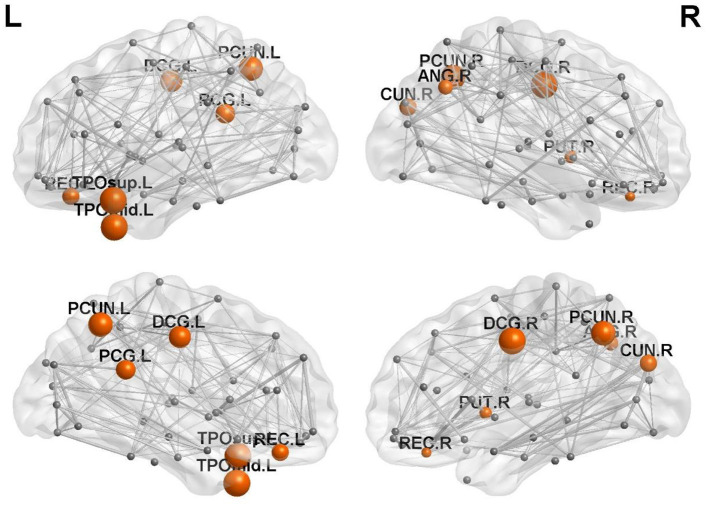
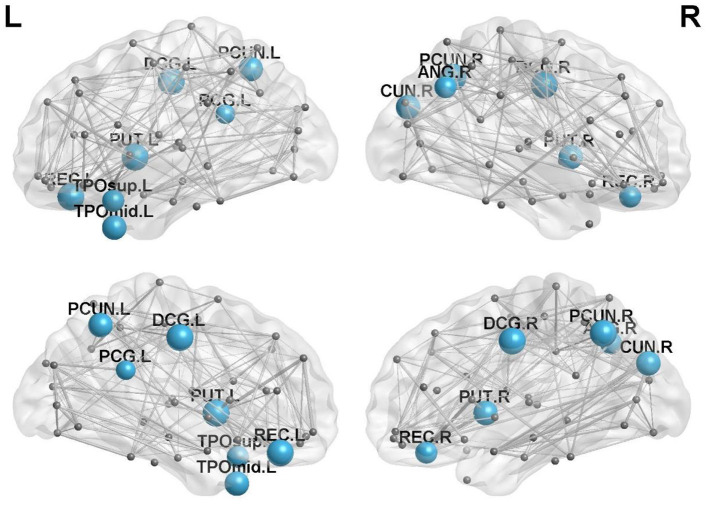
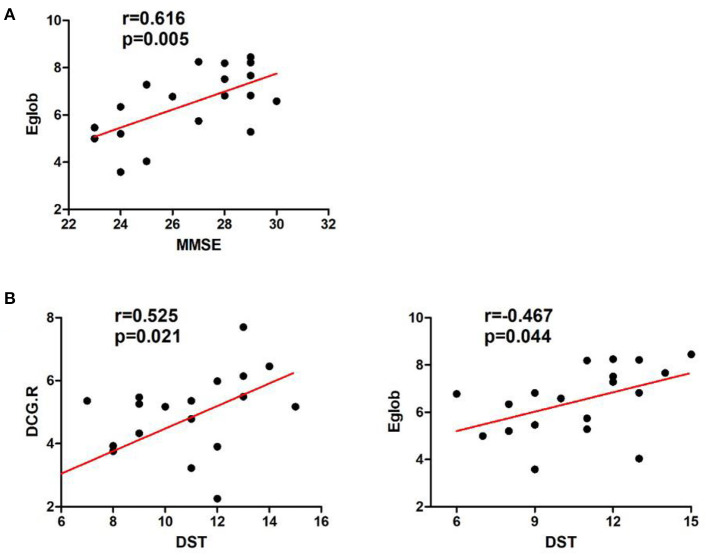
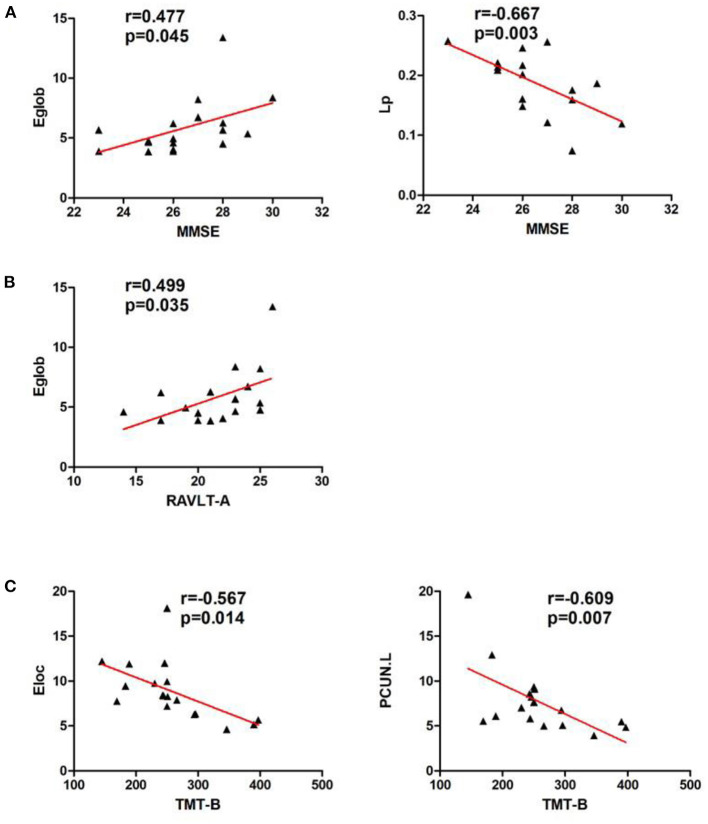
Results: The Mini-Mental Status Examination (MMSE), Montreal Cognitive Assessment (MOCA) and the Rey auditory verbal learning test (RAVLT) scores in the left and right cerebellar infarction groups were significantly lower than those in the healthy control group (p < 0.05). In addition, the digit span test (DST) scores were lower in the left cerebellar infarction group (p < 0.05); the trail-making test (TMT) times in the right cerebellar infarction group were significantly higher than those in the left cerebellar infarction group (p < 0.05). Meanwhile, the left and right cerebellar infarction groups had abnormal brain topological properties, including clustering coefficient, shortest path length, global efficiency, local efficiency and nodal efficiency. After unilateral cerebellar infarction, bilateral cerebral nodal efficiency was abnormal. Correlation analysis showed that there was a close correlation between decreased processing speed in patients with left cerebellar infarction and decreased efficiency of right cerebral nodes (p < 0.05), and there was a close relationship between executive dysfunction and decreased efficiency of left cerebral nodes in patients with right cerebellar infarction (p < 0.05).
Conclusion: Patients with cerebellar infarction have cognitive impairment. Unilateral cerebellar infarction can reduce the network efficiency of key regions in the bilateral cerebral hemispheres, and these abnormal changes are closely related to patient cognitive impairment. The results of this study provide evidence for understanding the underlying neural mechanisms of cerebellar cognitive impairment and suggest that brain topological network properties may be markers of cerebellar cognitive impairment.
Keywords: brain network; cerebellar infarction; cognitive impairment; diffusion tensor imaging; graph theory.
Copyright © 2022 Wang, Yao, Lin, Hu and Shi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources