

Multiomic characterization and drug testing establish circulating tumor cells as an ex vivo tool for personalized medicine
- PMID: 36204272
- PMCID: PMC9529671
- DOI: 10.1016/j.isci.2022.105081
Multiomic characterization and drug testing establish circulating tumor cells as an ex vivo tool for personalized medicine
Abstract
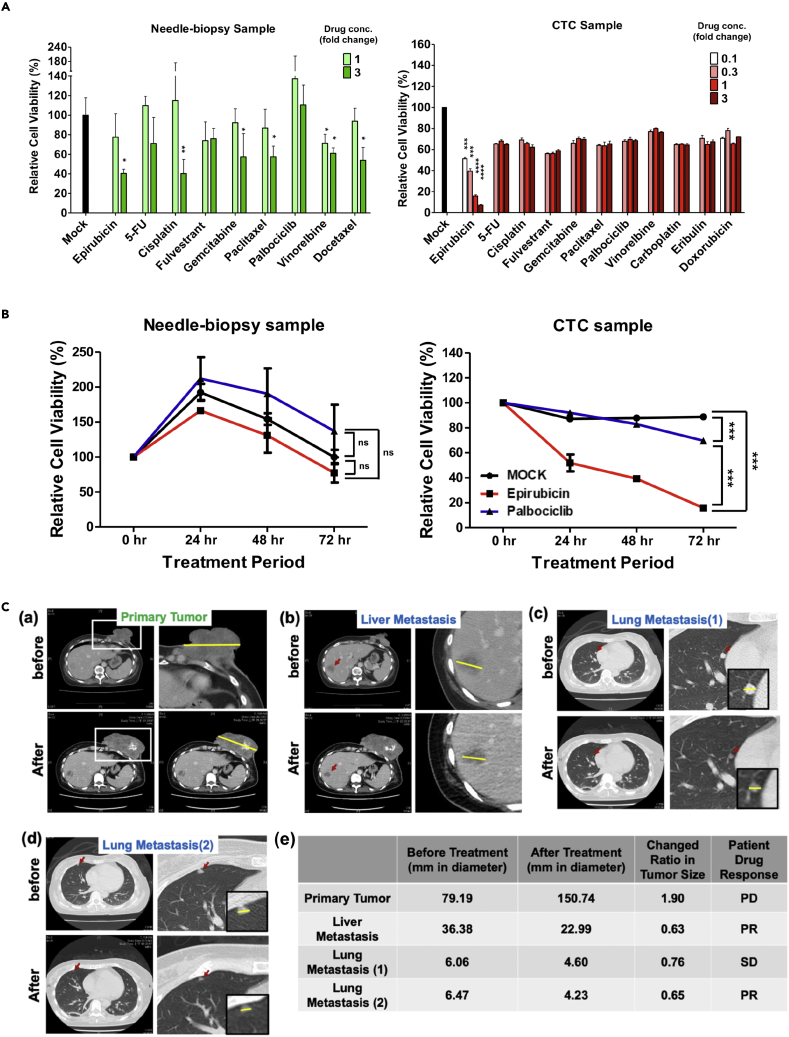
Matching the treatment to an individual patient's tumor state can increase therapeutic efficacy and reduce tumor recurrence. Circulating tumor cells (CTCs) derived from solid tumors are promising subjects for theragnostic analysis. To analyze how CTCs represent tumor states, we established cell lines from CTCs, primary and metastatic tumors from a mouse model and provided phenotypic and multiomic analyses of these cells. CTCs and metastatic cells, but not primary tumor cells, shared stochastic mutations and similar hypomethylation levels at transcription start sites. CTCs and metastatic tumor cells shared a hybrid epithelial/mesenchymal transcriptome state with reduced adhesive and enhanced mobilization characteristics. We tested anti-cancer drugs on tumor cells from a metastatic breast cancer patient. CTC responses mirrored the impact of drugs on metastatic rather than primary tumors. Our multiomic and clinical anti-cancer drug response results reveal that CTCs resemble metastatic tumors and establish CTCs as an ex vivo tool for personalized medicine.
Keywords: Cancer; Omics; Precision medicine; Transcriptomics.
© 2022 The Authors.
Conflict of interest statement
Ying-Chih Chang is the founder and stockholder of Acrocyte Therapeutics Inc., New Taipei City, Taiwan. Other authors declare no conflicts of interest.
Figures







References
-
- Aceto N., Toner M., Maheswaran S., Haber D.A. En route to metastasis: circulating tumor cell clusters and epithelial-to-mesenchymal transition. Trends Cancer. 2015;1:44–52. - PubMed
-
- Bidard F.C., Jacot W., Kiavue N., Dureau S., Kadi A., Brain E., Bachelot T., Bourgeois H., Gonçalves A., Ladoire S., et al. Efficacy of circulating tumor cell count-driven vs clinician-driven first-line therapy choice in hormone receptor-positive, ERBB2-negative metastatic breast cancer: the STIC CTC randomized clinical trial. JAMA Oncol. 2021;7:34–41. doi: 10.1001/jamaoncol.2020.5660. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
