

Importance of Delayed Reperfusions in Patients With Incomplete Thrombectomy
- PMID: 36205143
- PMCID: PMC9586830
- DOI: 10.1161/STROKEAHA.122.040063
Importance of Delayed Reperfusions in Patients With Incomplete Thrombectomy
Abstract
Background: There is paucity of data regarding the effects of delayed reperfusion (DR) on clinical outcomes in patients with incomplete reperfusion following mechanical thrombectomy. We hypothesized that DR has a strong association with clinical outcome in patients with incomplete reperfusion after mechanical thrombectomy (expanded Thrombolysis in Cerebral Infarction, 2a-2c).
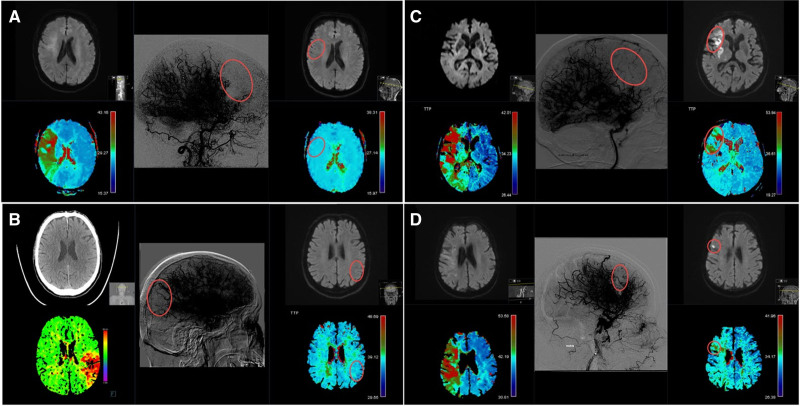
Methods: Single-institution's stroke registry retrospective analysis of patients admitted from February 2015 to December 2020. DR was defined as the absence of any perfusion delay on ≈24-hour contrast-enhanced follow-up perfusion imaging, whereas persistent perfusion deficit denotes a perfusion delay corresponding to the catheter angiographic deficit directly after the intervention. The association of perfusion outcome (DR versus persistent perfusion deficit) with the occurrence of new infarcts and 90-day functional independence (modified Rankin Scale score 0-2) was evaluated using logistic regression analyses. Comparison of predictive accuracy was evaluated by calculating area under the curve for models with and without perfusion outcome.
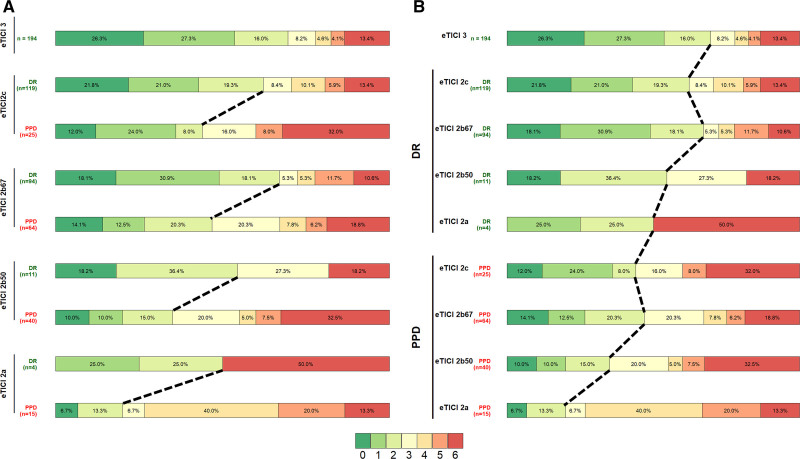
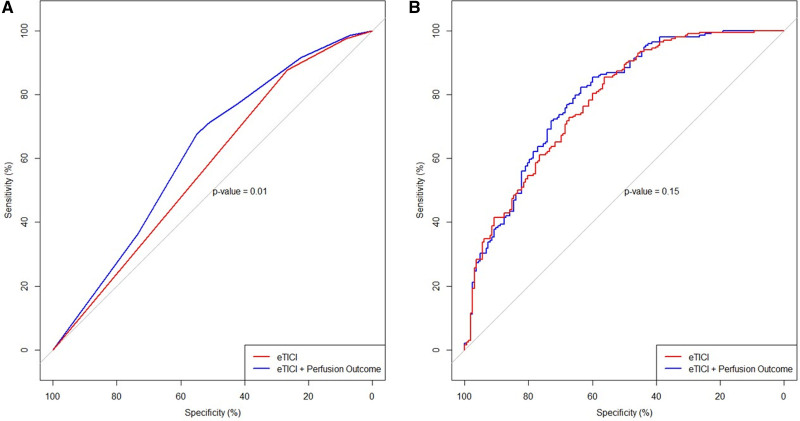
Results: In 566 patients (mean age 74, 49.6% female), new infarcts in the incomplete reperfusion areas were less common in DR versus persistent perfusion deficit patients (small punctiform: 17.1% versus 25%, large confluent: 7.9% versus 63.2%; P=0.001). After adjustment for confounders, DR was a strong predictor of functional independence (adjusted odds ratio, 2.37 [95% CI 1.34-4.23]). There was a significant improvement in predictive accuracy of functional independence when perfusion outcome was added to expanded Thrombolysis in Cerebral Infarction alone (area under the curve 0.57 versus 0.62, P=0.01).
Conclusions: Occurrence of DR is closely associated with tissue outcome and functional independence. DR may be an independent prognostic parameter, suggesting it as a potential outcome surrogate for medical rescue therapies.
Keywords: ischemic stroke; magnetic resonance imaging; reperfusion; thrombectomy; tomography.
Figures
References
-
- Tachibana M, Ago T, Wakisaka Y, Kuroda J, Shijo M, Yoshikawa Y, Komori M, Nishimura A, Makihara N, Nakamura K, et al. Early reperfusion after brain ischemia has beneficial effects beyond rescuing neurons. Stroke. 2017;48:2222–2230. doi: 10.1161/STROKEAHA.117.016689 - PubMed
-
- Yoo AJ, Soomro J, Andersson T, Saver JL, Ribo M, Bozorgchami H, Dabus G, Liebeskind DS, Jadhav A, Mattle H, et al. Benchmarking the extent and speed of reperfusion: first pass TICI 2c-3 is a preferred endovascular reperfusion endpoint. Front Neurol. 2021;12:669934. doi: 10.3389/fneur.2021.669934 - PMC - PubMed
-
- Hill MD, Goyal M, Menon BK, Nogueira RG, McTaggart RA, Demchuk AM, Poppe AY, Buck BH, Field TS, Dowlatshahi D, et al. ; ESCAPE-NA1 Investigators. Efficacy and safety of nerinetide for the treatment of acute ischaemic stroke (ESCAPE-NA1): a multicentre, double-blind, randomised controlled trial. Lancet. 2020;395:878–887. doi: 10.1016/S0140-6736(20)30258-0 - PubMed
-
- Leischner H, Flottmann F, Hanning U, Broocks G, Faizy TD, Deb-Chatterji M, Bernhardt M, Brekenfeld C, Buhk JH, Gellissen S, et al. Reasons for failed endovascular recanalization attempts in stroke patients. J Neurointerv Surg. 2019;11:439–442. doi: 10.1136/neurintsurg-2018-014060 - PubMed
