

Three-Year Interval for the Multi-Target Stool DNA Test for Colorectal Cancer Screening: A Longitudinal Study
- PMID: 36205504
- PMCID: PMC9900315
- DOI: 10.1158/1940-6207.CAPR-22-0238
Three-Year Interval for the Multi-Target Stool DNA Test for Colorectal Cancer Screening: A Longitudinal Study
Abstract
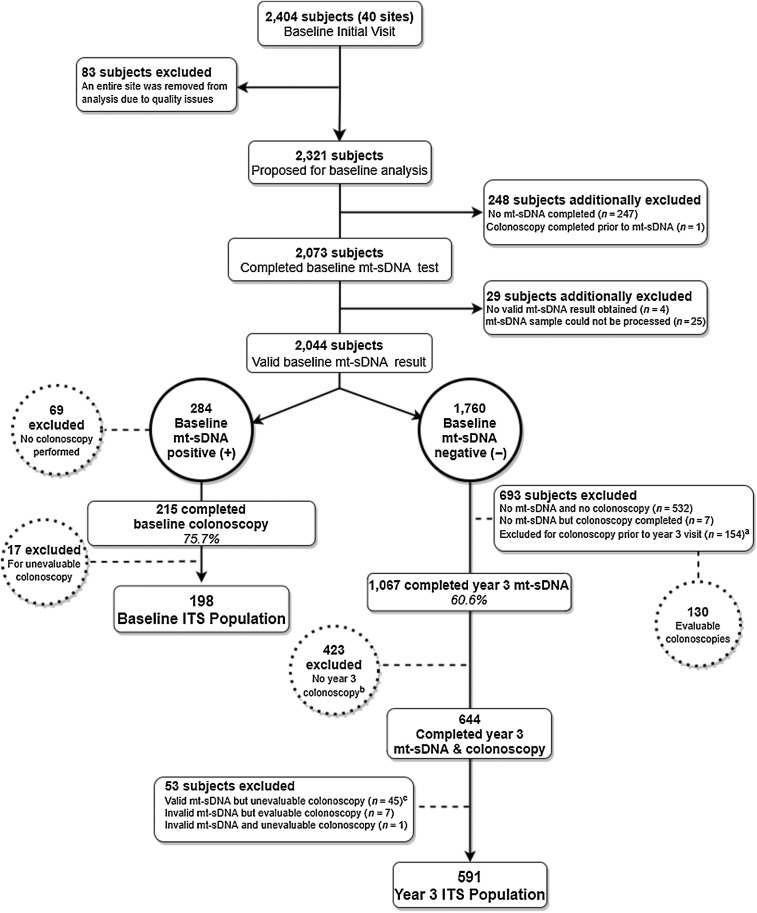
Data supporting the clinical utility of multi-target stool DNA (mt-sDNA) at the guideline-recommended 3-year interval have not been reported.Between April 2015 and July 2016, candidates for colorectal cancer screening whose providers prescribed the mt-sDNA test were enrolled. Participants with a positive baseline test were recommended for colonoscopy and completed the study. Those with a negative baseline test were followed annually for 3 years. In year 3, the mt-sDNA test was repeated and colonoscopy was recommended independent of results. Data were analyzed using the Predictive Summary Index (PSI), a measure of the gain in certainty for dichotomous diagnostic tests (where a positive value indicates a net gain), and by comparing observed versus expected colorectal cancers and advanced precancerous lesions.Of 2,404 enrolled subjects, 2,044 (85%) had a valid baseline mt-sDNA result [284 (13.9%) positive and 1,760 (86.1%) negative]. Following participant attrition, the year 3 intention to screen cohort included 591 of 1,760 (33.6%) subjects with valid mt-sDNA and colonoscopy results, with no colorectal cancers and 63 advanced precancerous lesions [22 (34.9%) detected by mt-sDNA] and respective PSI values of 0% (P = 1) and 9.3% (P = 0.01). The observed 3-year colorectal cancer yield was lower than expected (one-sided P = 0.09), while that for advanced precancerous lesions was higher than expected (two-sided P = 0.009).Repeat mt-sDNA screening at a 3-year interval resulted in a statistically significant gain in detection of advanced precancerous lesions. Due to absence of year 3 colorectal cancers, the PSI estimate for colorectal cancer was underpowered and could not be reliably quantified. Larger studies are required to assess the colorectal cancer study findings.
Prevention relevance: Understanding the 3-year yield of mt-sDNA for colorectal cancer and advanced precancerous polyps is required to ensure the clinical appropriateness of the 3-year interval and to optimize mt-sDNA's screening effectiveness.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- American Cancer Society. ACS Facts and Figures 2022. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-....
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7–33. - PubMed
-
- American Cancer Society. When should you start getting screened for colorectal cancer? 2021. Available from: https://www.cancer.org/latest-news/american-cancer-society-updates-color....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
