

Progression of Low-Risk Papillary Thyroid Microcarcinoma During Active Surveillance: Interim Analysis of a Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma in Korea
- PMID: 36205563
- PMCID: PMC9700369
- DOI: 10.1089/thy.2021.0614
Progression of Low-Risk Papillary Thyroid Microcarcinoma During Active Surveillance: Interim Analysis of a Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma in Korea
Abstract
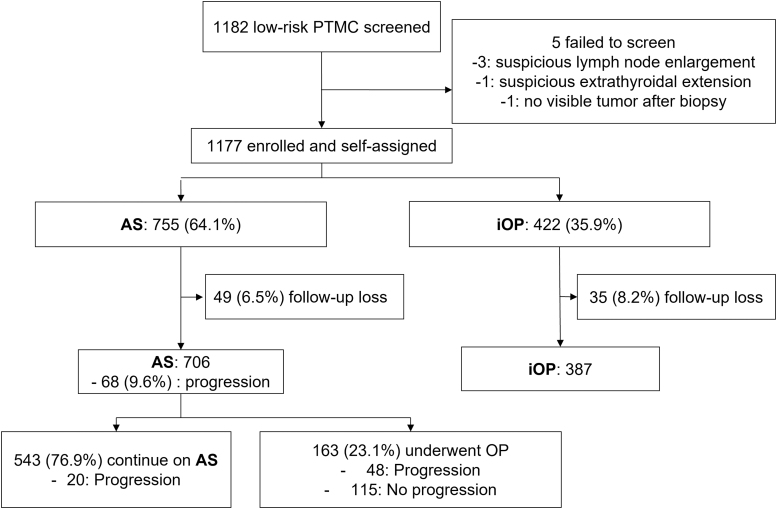
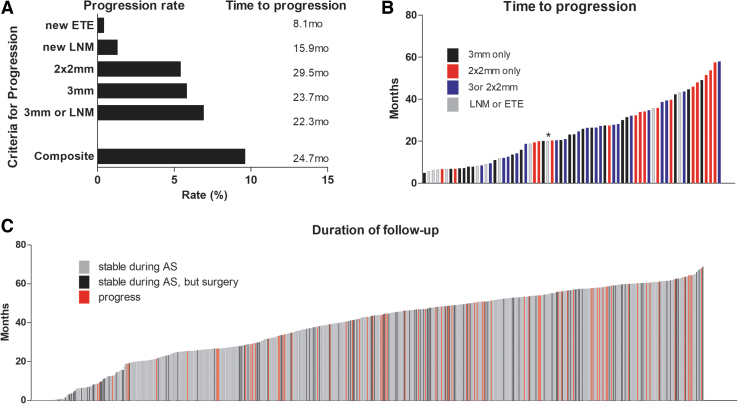
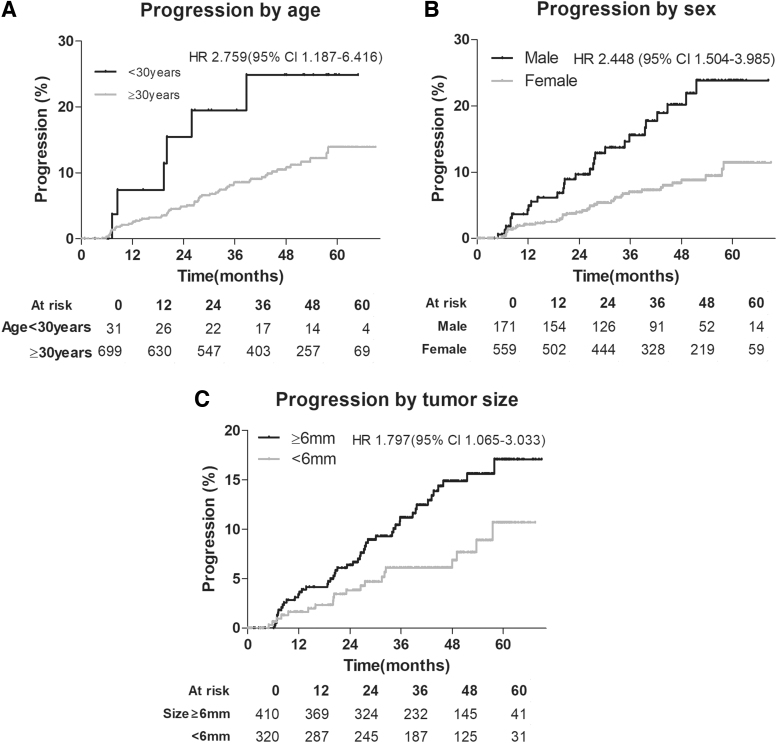
Background: Active surveillance (AS) is an alternative to thyroidectomy for the management of low-risk papillary thyroid microcarcinoma (PTMC). However, prospective AS data collected from diverse populations are needed. Methods: This multicenter prospective cohort study enrolled patients from three referral hospitals in Korea. The participants were self-assigned into two groups, AS or immediate surgery. All patients underwent neck ultrasound every 6-12 months to monitor for disease progression. Progression under AS was evaluated by a criterion of tumor size increment by 3 mm in one dimension (3 mm), 2 mm in two dimensions (2 × 2 mm), new extrathyroidal extension (ETE), or new lymph node metastasis (LNM), and a composite outcome was defined using all four criteria. Results: A total of 1177 eligible patients with PTMC (919 female, 78.1%) with a median age of 48 years (range 19-87) were enrolled; 755 (64.1%) patients chose AS and 422 (35.9%) underwent surgery. Among 755 patients under AS, 706 (female 537, 76.1%) underwent at least two ultrasound examinations and were analyzed. Over a follow-up period of 41.4 months (standard deviation, 16.0), 163 AS patients (23.1%) underwent surgery. Progression defined by the composite outcome was observed in 9.6% (68/706) of patients, and the 2- and 5-year progression estimates were 5.3% and 14.2%, respectively. The observed progression rates were 5.8% (41/706) and 5.4% (38/706) as defined by tumor size enlargement by 3 mm and 2 × 2 mm, respectively, and 1.3% (9/706) and 0.4% (3/706) for new LNM and ETE, respectively. No distant metastases developed during AS. In multivariate logistic regression analysis examining variables associated with progression under AS, age at diagnosis <30 years (odds ratio [OR], 2.86; 95% confidence interval [CI], 1.10 - 7.45), male sex (OR, 2.48; 95% CI, 1.47 - 4.20), and tumor size ≥6 mm (OR, 1.89; 95% CI, 1.09 - 3.27) were independently significant. Conclusions: The progression of low-risk PTMC during AS in the Korean population was low, but slightly higher than previously reported in other populations. Risk factors for disease progression under AS include younger age, male sex, and larger tumor size. Clinical trial registration: Clinicaltrials.gov NCT02938702.
Keywords: active surveillance; immediate surgery; microcarcinoma; papillary; thyroid cancer; thyroidectomy; watchful waiting.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Thyroid Cancer Active Surveillance: The Devil You Know or The Devil You Don't.Thyroid. 2022 Nov;32(11):1279-1280. doi: 10.1089/thy.2022.0541. Epub 2022 Nov 4. Thyroid. 2022. PMID: 36205589 No abstract available.
References
Publication types
MeSH terms
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials