

Association of Early Norepinephrine Administration With 24-Hour Mortality Among Patients With Blunt Trauma and Hemorrhagic Shock
- PMID: 36205999
- PMCID: PMC9547317
- DOI: 10.1001/jamanetworkopen.2022.34258
Association of Early Norepinephrine Administration With 24-Hour Mortality Among Patients With Blunt Trauma and Hemorrhagic Shock
Abstract
Importance: Hemorrhagic shock is a common cause of preventable death after injury. Vasopressor administration for patients with blunt trauma and hemorrhagic shock is often discouraged.
Objective: To evaluate the association of early norepinephrine administration with 24-hour mortality among patients with blunt trauma and hemorrhagic shock.
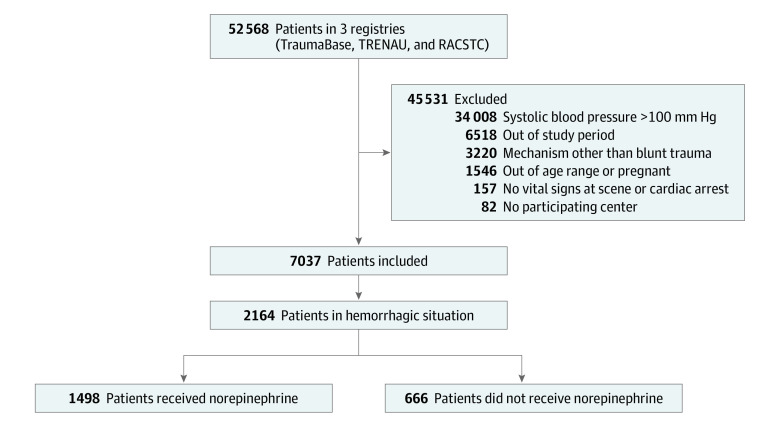
Design, setting, and participants: This retrospective, multicenter, observational cohort study used data from 3 registries in the US and France on all consecutive patients with blunt trauma from January 1, 2013, to December 31, 2018. Patients were alive on admission with hemorrhagic shock, defined by prehospital or admission systolic blood pressure less than 100 mm Hg and evidence of hemorrhage (ie, prehospital or resuscitation room transfusion of packed red blood cells, receipt of emergency treatment for hemorrhage control, transfusion of >10 units of packed red blood cells in the first 24 hours, or death from hemorrhage). Blunt trauma was defined as any exposure to nonpenetrating kinetic energy, collision, or deceleration. Statistical analysis was performed from January 15, 2021, to February 22, 2022.
Exposure: Continuous administration of norepinephrine in the prehospital environment or resuscitation room prior to hemorrhage control, according to European guidelines.
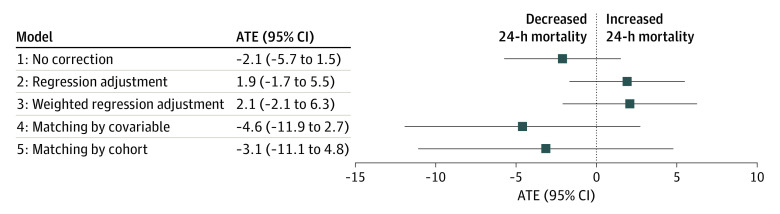
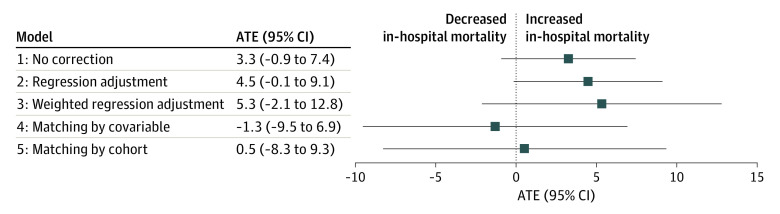
Main outcomes and measures: The primary outcome was 24-hour mortality, and the secondary outcome was in-hospital mortality. The average treatment effect (ATE) of early norepinephrine administration on 24-hour mortality was estimated according to the Rubin causal model. Inverse propensity score weighting and the doubly robust approach with 5 distinct analytical strategies were used to determine the ATE.
Results: A total of 52 568 patients were screened for inclusion, and 2164 patients (1508 men [70%]; mean [SD] age, 46 [19] years; median Injury Severity Score, 29 [IQR, 17-36]) presented with acute hemorrhage and were included. A total of 1497 patients (69.1%) required emergency hemorrhage control, 128 (5.9%) received a prehospital transfusion of packed red blood cells, and 543 (25.0%) received a massive transfusion. Norepinephrine was administered to 1498 patients (69.2%). The 24-hour mortality rate was 17.8% (385 of 2164), and the in-hospital mortality rate was 35.6% (770 of 2164). None of the 5 analytical strategies suggested any statistically significant association between norepinephrine administration and 24-hour mortality, with ATEs ranging from -4.6 (95% CI, -11.9 to 2.7) to 2.1 (95% CI, -2.1 to 6.3), or between norepinephrine administration and in-hospital mortality, with ATEs ranging from -1.3 (95% CI, -9.5 to 6.9) to 5.3 (95% CI, -2.1 to 12.8).
Conclusions and relevance: The findings of this study suggest that early norepinephrine infusion was not associated with 24-hour or in-hospital mortality among patients with blunt trauma and hemorrhagic shock. Randomized clinical trials that study the effect of early norepinephrine administration among patients with trauma and hypotension are warranted to further assess whether norepinephrine is safe for patients with hemorrhagic shock.
Conflict of interest statement
Figures
References
-
- CRASH-2 collaborators; Roberts I, Shakur H, Afolabi A, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-1101, 1101.e1-2. doi:10.1016/S0140-6736(11)60278-X - DOI - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, et al. ; PROPPR Study Group . Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471-482. doi:10.1001/jama.2015.12 - DOI - PMC - PubMed
-
- Pusateri AE, Moore EE, Moore HB, et al. . Association of prehospital plasma transfusion with survival in trauma patients with hemorrhagic shock when transport times are longer than 20 minutes: a post hoc analysis of the PAMPer and COMBAT clinical trials. JAMA Surg. 2020;155(2):e195085. doi:10.1001/jamasurg.2019.5085 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
