

Lorlatinib and compound mutations in ALK+ large-cell neuroendocrine lung carcinoma: a case report
- PMID: 36207130
- PMCID: PMC9632356
- DOI: 10.1101/mcs.a006234
Lorlatinib and compound mutations in ALK+ large-cell neuroendocrine lung carcinoma: a case report
Abstract
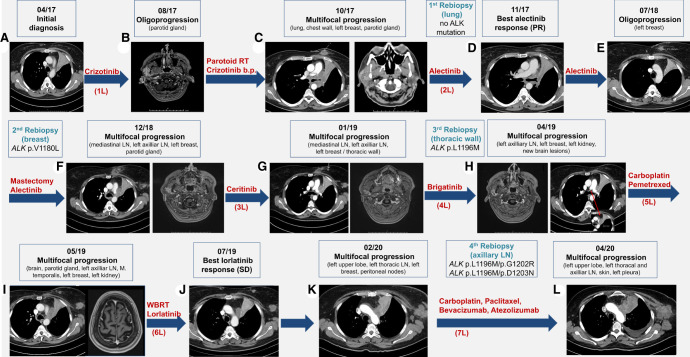
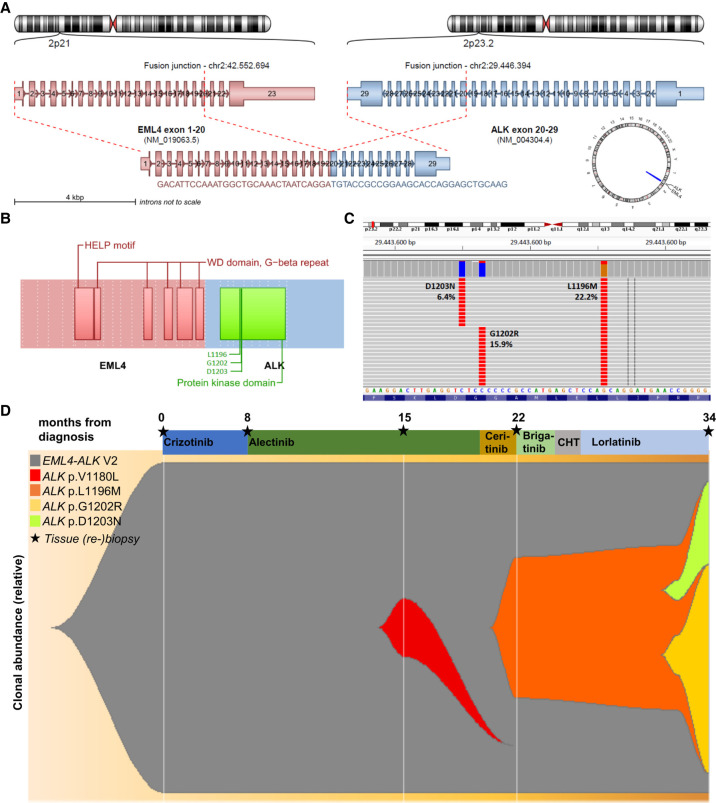
Large-cell neuroendocrine lung carcinoma (LCNEC) is a high-grade neoplasm with median survival of 1 year and limited therapeutic options. Here, we report the unusual case of a 47-yr-old female smoker with stage IV LCNEC featuring EML4-ALK variant 2 (E20:A20), wild-type TP53/RB1, and low tumor mutational burden of 3.91 mut/Mb. Despite early progression within 3 mo under crizotinib, a durable response was achieved with alectinib. Oligoprogression in the left breast 10 mo later was treated by surgery, followed by a switch to ceritinib upon multifocal progression and detection of ALK:p.V1180L in the mastectomy specimen, but without success. Another rebiopsy revealed ALK:p.L1196M, but the tumor did not respond to brigatinib or carboplatin/pemetrexed, before stabilization under lorlatinib. Diffuse progression 8 mo later with detection of ALK :p.L1196M/p.G1202R and p.L1196M/ p.D1203N evolving from the previous p.L1196M did not respond to chemoimmunotherapy, and the patient succumbed with an overall survival (OS) of 37 mo. This case illustrates the importance of molecular profiling for LCNEC regardless of smoking status, and the superiority of next-generation ALK inhibitors compared to crizotinib for ALK+ cases. Lorlatinib retained efficacy in the heavily pretreated setting, whereas its upfront use could possibly have prevented the stepwise emergence of compound ALK mutations. Furthermore, the disease course was more aggressive and OS shorter compared to the V2/TP53wt ALK+ lung adenocarcinoma, whereas crizotinib, ceritinib, and brigatinib did not confer the benefit expected according to next-generation sequencing results, which also underline the need for more potent drugs against ALK in the high-risk setting of neuroendocrine histology.
Keywords: lung adenocarcinoma.
© 2022 Wiedemann et al.; Published by Cold Spring Harbor Laboratory Press.
Figures
References
-
- Angeles AK, Christopoulos P, Yuan Z, Bauer S, Janke F, Ogrodnik SJ, Reck M, Schlesner M, Meister M, Schneider MA, et al. 2021. Early identification of disease progression in ALK-rearranged lung cancer using circulating tumor DNA analysis. NPJ Precis Oncol 5: 100. 10.1038/s41698-021-00239-3 - DOI - PMC - PubMed
-
- Camidge DR, Kim HR, Ahn MJ, Yang JCH, Han JY, Hochmair MJ, Lee KH, Delmonte A, Campelo MRG, Kim DW, et al. 2021. Brigatinib versus crizotinib in ALK inhibitor-naive advanced ALK-positive NSCLC: final results of phase 3 ALTA-1L trial. J Thor Dis 16: 2091–2108. 10.1016/j.jtho.2021.07.035 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous